

Jarrow Formulas
B-12 & Folate Extra Strength Lemon by Jarrow Formulas
100 chewable tablets
Support Energy Production and Healthy Cell Function with B-12 and Folate$23.99retail
Add to cart for 21% off
Purchase option
21% below MSRP3rd-party tested for purity & potencyFree shipping $50+
Vegan·Vegetarian·Gluten Free·Soy Free·Dairy Free·Milk Free·
Jarrow Formulas B-12 & Folate Extra Strength Lemon overview
If you are searching for methyl B12 and methylfolate because your energy is low or labs show gaps, this combo fits a real need. It suits vegans and vegetarians, metformin users, people on acid blockers, and anyone with low Vitamin B12, low Folate, or elevated Homocysteine (an amino acid tied to vascular risk). It is also useful if your Methylmalonic Acid (a functional marker of B12 status) runs high. The 1,000 mcg methyl B12 here is a maintenance-level dose for low-normal labs; established deficiency, bariatric surgery, or pernicious anemia usually require higher-dose or injectable B12 under clinician care.
Methylcobalamin (the active form of B12) and 5-MTHF (the active form of folate) donate methyl groups that run methylation, the body’s tagging system for building neurotransmitters and regulating gene expression. Together they recycle Homocysteine back to methionine, which often lowers Homocysteine in 4 to 8 weeks in responders. Pyridoxal 5-phosphate (P5P, active B6) helps convert excess Homocysteine into cysteine through the transsulfuration pathway (a detox route for sulfur amino acids). Compared with cyanocobalamin or folic acid, these active forms bypass common genetic bottlenecks and are well absorbed when dissolved in the mouth.
Dissolve or chew one lemon tablet daily, with or without food. Morning works best for most; if you are sensitive to B12, avoid taking it late in the day. Sublingual absorption (in the mouth) can help if stomach acid is low. Recheck Vitamin B12, Folate, and Homocysteine after 8 to 12 weeks. If your levels remain low, a higher-dose B12 lozenge or injections are more practical than adding multiple tablets.
If you have neurologic symptoms from B12 deficiency (numbness, balance changes), see a clinician first. Pernicious anemia needs supervised therapy and often injections. High-dose methotrexate for cancer conflicts with folate; do not self-supplement without oncology approval. Phenytoin and some anti-seizure drugs can be affected by folate. Metformin and proton-pump inhibitors commonly lower B12 over time, so pairing this B12 with periodic Vitamin B12 and Methylmalonic Acid testing is sensible. Pregnancy requires daily folate, but use it within a full prenatal plan.
Frequently asked questions
How long does methyl B12 and methylfolate take to work?
Energy changes are often noticed within 1 to 3 weeks, but lab shifts take longer. Homocysteine typically responds within 4 to 8 weeks, and Vitamin B12 or Folate levels usually rise on repeat testing within 8 to 12 weeks.
Is 1,000 mcg of B12 enough?
For low-normal Vitamin B12 or prevention in higher-risk groups, 1,000 mcg daily is a common maintenance dose. If you have clear deficiency, neurological symptoms, bariatric surgery, or pernicious anemia, you likely need higher doses or injections under medical guidance.
Should I take B12 and folate together or separately?
Together is reasonable. B12 and methylfolate work on the same methylation cycle that recycles Homocysteine. Adding active B6 (P5P) helps the parallel pathway that disposes of Homocysteine, which is why this three-in-one formula is practical.
Can B12 keep me awake if I take it at night?
It can in some people. B12 is involved in neurotransmitter production and circadian signaling, so take it in the morning if you notice restlessness or vivid dreams when dosing later in the day.
What labs should I check with B12 and folate?
Start with Vitamin B12, Folate, and Homocysteine. Add Methylmalonic Acid if B12 status is unclear and a Complete Blood Count to review MCV (average red cell size). Recheck 8 to 12 weeks after consistent use.
Does methyl B12 lower Homocysteine on its own?
Sometimes, but results are more consistent with both methylfolate and B6 on board. This combination addresses recycling and disposal routes for Homocysteine, which improves the odds of a meaningful drop.
Is methylfolate better than folic acid for MTHFR variants?
For people with reduced MTHFR enzyme activity, 5-MTHF is the already-active form and bypasses that step. It is a practical choice if your Homocysteine is elevated or you have a history of low Folate despite taking folic acid.
How to take it & ingredients
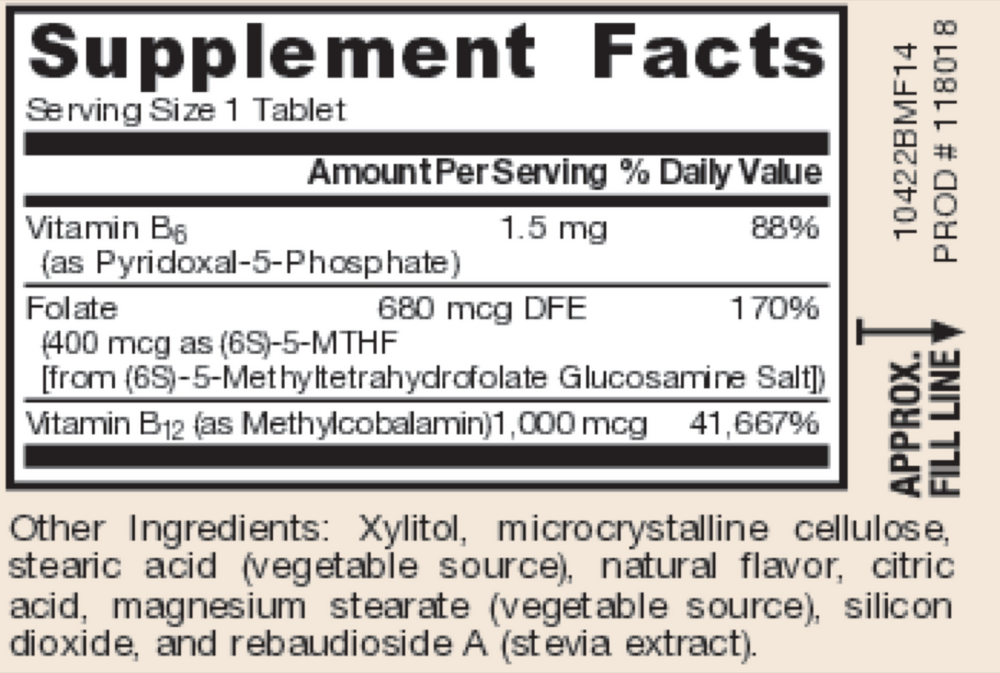
Suggested use: Dissolve in mouth or chew 1 tablet per day or as directed by your qualified healthcare professional.
Active ingredients
1 tablet per serving
Vitamin B6
Pyridoxal 5-Phosphate
Pyridoxal 5-Phosphate
1.5 mg
Folate
(6S)-5-MTHF [from Quatrefolic® (6S)-5-methyltetrahydrofolate glucosamine salt]
(6S)-5-MTHF [from Quatrefolic® (6S)-5-methyltetrahydrofolate glucosamine salt]
400 mcg
Vitamin B12
Methylcobalamin
Methylcobalamin
1000 mcg
Other ingredients: Xylitol, Cellulose, Stearic acid (vegetable source), Natural cherry flavor, Citric acid, Organic rebiana (stevia) extract, Magnesium stearate (vegetable source)
Certifications
Benefits
Warnings