
Theralogix
Prosteon Bone Health Supplement by Theralogix
360 tablets
Comprehensive Support for Strong Bones and Healthy Aging$64.99retail
Add to cart for 20% off
Purchase option
20% below MSRP3rd-party tested for purity & potencyFree shipping $50+
Vegetarian·Gluten Free
Theralogix Prosteon Bone Health Supplement overview
If your Vitamin D, 25-Hydroxy is in the lower end of normal, your DXA scan (a low-dose X‑ray of bone density) shows decline, or you get little calcium from food, calcium citrate is a practical base. It’s also a smart add‑on for men on androgen‑deprivation therapy, who lose bone faster. The 500 mg here covers roughly half of a typical daily calcium target, so it pairs well with a calcium‑aware diet. If you’re repleting a clear vitamin D deficiency, you’ll likely need a higher D3 dose short‑term, then step down.
Calcium citrate absorbs well even if stomach acid is low, and vitamin D3 improves calcium uptake while helping keep parathyroid hormone (the signal that pulls calcium from bone) in check. Vitamin K2 as MK‑4 activates osteocalcin (a bone protein that guides calcium into the matrix), which helps keep calcium in bone rather than soft tissues. Magnesium supports the bone scaffold, and boron improves vitamin D activity and calcium handling. In practice, bone turnover markers like P1NP and CTX (blood tests of bone building and breakdown) can shift within 3–6 months; density changes take longer on DXA.
Take two tablets daily with food, or split across meals if your stomach is sensitive. Calcium blocks absorption of levothyroxine (thyroid hormone) and some antibiotics, so separate by at least 4 hours. If you also take iron, take it at a different meal. This is a maintenance‑level vitamin D3 dose; if your Vitamin D, 25‑Hydroxy is low, confirm repletion with follow‑up labs within 8–12 weeks.
If you use warfarin (a blood thinner that blocks vitamin K), avoid vitamin K2 unless your prescriber adjusts your dose and monitors INR (a clotting test). Post‑parathyroid or sarcoid patients prone to high calcium, and those with active kidney stones or advanced kidney disease, should review serum calcium and 24‑hour urine results with a clinician before adding calcium. If you’re starting bisphosphonates (drugs that slow bone loss), calcium and D3 remain foundational but must be timed away from the pill.
Is calcium citrate better than carbonate? It’s easier to absorb and gentler on the stomach, especially with low stomach acid. How long until results? Expect changes in bone markers within 3–6 months and DXA changes over 12 months or more. Using Theralogix Prosteon alongside exercise and adequate protein typically works better than pills alone.
Frequently asked questions
Is calcium citrate better than calcium carbonate?
For many adults, yes. Calcium citrate absorbs well with or without meals and is gentler if stomach acid is low or if you use acid‑reducing meds. Carbonate is fine for some, but it requires more stomach acid and is more often linked to gas and bloating.
How long does a bone health supplement take to work?
Biochemistry shifts first: bone turnover markers like P1NP and CTX can change in 3–6 months. Measurable bone density changes on DXA usually take 12 months or longer. Keep intake steady and recheck labs and DXA on a schedule your clinician sets.
Can I take this with osteoporosis medications like alendronate?
Yes, but separate dosing. Take alendronate on an empty stomach first thing, then wait at least 30 minutes (often longer per your doctor) before food or supplements. Calcium taken too close blocks drug absorption. Calcium and D3 are still foundational with these meds.
Does vitamin K2 interact with blood thinners?
With warfarin, yes. Vitamin K2 opposes warfarin’s effect, so avoid it unless your prescriber adjusts the dose and monitors INR closely. Newer blood thinners (like apixaban or rivaroxaban) don’t rely on vitamin K and aren’t affected the same way.
Will calcium citrate cause kidney stones?
Taken with meals, calcium citrate can actually lower urinary oxalate and is often preferred in people with calcium‑oxalate stones. That said, if you have a stone history, coordinate intake with a clinician using 24‑hour urine testing to calibrate dose and timing.
Is 1,000 IU of vitamin D3 enough?
It’s a maintenance dose for many adults. If your Vitamin D, 25‑Hydroxy is low, short‑term higher dosing is usually needed, followed by retesting in 8–12 weeks and stepping down. Body weight, sun exposure, and skin tone all influence needs.
When should I take calcium relative to thyroid medication?
Separate by at least 4 hours. Calcium binds levothyroxine in the gut and reduces absorption. The same spacing rule applies to iron and certain antibiotics (like tetracyclines and quinolones).
Who especially benefits from this bone health supplement?
Adults with low dietary calcium, low‑normal Vitamin D, or documented bone loss on DXA, and men on androgen‑deprivation therapy. Strength training and adequate protein amplify the benefit beyond supplementation alone.
How to take it & ingredients
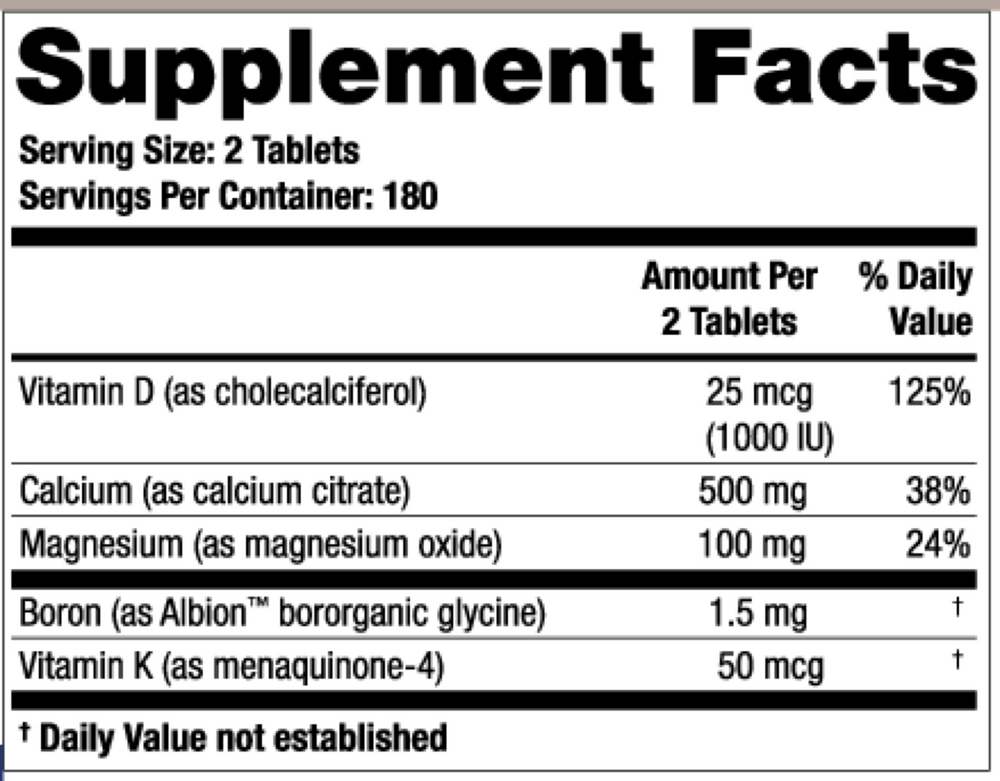
Suggested use: Adults take two tablets daily, with food, or as directed by your healthcare professional.
Active ingredients
2 tablets per serving
Vitamin D
Cholecalciferol (Vitamin D3)
Cholecalciferol (Vitamin D3)
25 mcg, 1000 IU
Calcium
Calcium Citrate
Calcium Citrate
500 mg
Magnesium
Magnesium Malate
Magnesium Malate
100 mg
Boron
Albon™ Bororganic Glycine
Albon™ Bororganic Glycine
1.5 mg
Vitamin K
Menaquinone-4
Menaquinone-4
50 mcg
Other ingredients: Microcrystalline Cellulose, Croscarmellose Sodium, Vegetable Stearic Acid, Silicon Dioxide, Vegetable Magnesium Stearate, Clear Vegetable Coating (Hypromellose, Glycerine)
Certifications
Benefits
Warnings