

Thorne
5-Hydroxytryptophan by Thorne
90 capsules · 45-day supply
Supports Mood and Emotional Well-Being with 5-HTP and Vitamin B6$39.00retail
Add to cart for 21% off
Purchase option
21% below MSRP3rd-party tested for purity & potencyFree shipping $50+
Gluten Free·Soy Free·Dairy Free·Milk Free
Thorne 5-Hydroxytryptophan overview
If you’re searching for the best 5-HTP dose for sleep and find melatonin too groggy or short-acting, this fits. 5-HTP (5‑Hydroxytryptophan) is most useful for trouble falling asleep, low mood with carbohydrate cravings, and stress eating. The added vitamin B6 as P5P (the active form your enzymes use) helps your body convert 5-HTP efficiently. If your main issue is daytime fatigue rather than sleep onset, 5-HTP can feel sedating and may not be the right first step.
5-HTP crosses into the brain and is turned into serotonin (the neurotransmitter that steadies mood and appetite) by an enzyme that uses vitamin B6 as a cofactor. At night, some of that serotonin becomes melatonin (the sleep signal), which is why 5-HTP can ease sleep onset. Unlike tryptophan, it isn’t diverted into protein or niacin, so more goes toward serotonin. Many people notice calmer mood and fewer cravings within 1–2 weeks, and better sleep within the first few nights. Nausea happens when serotonin rises in the gut; taking with food usually solves it.
Thorne suggests 1–2 capsules three times daily. In practice, start low: 50–100 mg 30–60 minutes before bed for sleep. For mood or cravings, add 50–100 mg with breakfast and mid‑afternoon. Most people do well at 100–300 mg per day; higher intakes up to 300–600 mg are best done with a clinician. Take with a small snack to reduce nausea. If you’re tracking nutrients, “Vitamin B6, Plasma” can confirm you’re not low.
Skip 5-HTP if you take antidepressants that raise serotonin—SSRIs, SNRIs, MAOIs, or drugs like tramadol, linezolid, dextromethorphan, lithium, buspirone, or migraine triptans—or if you use St. John’s wort. Combining these raises the risk of serotonin syndrome (dangerous agitation, sweating, fast heart rate). Avoid in pregnancy or breastfeeding, with bipolar disorder (can trigger mania), carcinoid syndrome (already high serotonin), and with carbidopa for Parkinson’s.
People often ask if 5-HTP is better than melatonin. Use 5-HTP when mood and cravings matter alongside sleep; use melatonin when timing your body clock is the goal. Another question is labs—there’s no routine serotonin blood test to guide dosing, but checking Vitamin B6, Plasma is reasonable if you suspect deficiency.
Frequently asked questions
Does 5-HTP help you fall asleep?
Often yes. By raising serotonin that converts to melatonin at night, 5-HTP can shorten sleep onset. Many feel a difference within a few nights. If early awakenings are your main issue, it may help less than addressing sleep timing or light exposure.
How long does 5-HTP take to work?
Sleep effects can appear within 1–7 nights. Mood and craving changes usually build over 1–2 weeks of steady dosing. If you see no benefit by 3–4 weeks at 200–300 mg per day, reconsider the plan with a clinician.
Can I take 5-HTP with an SSRI or SNRI?
No. Combining 5-HTP with SSRIs, SNRIs, MAOIs, or triptans can cause serotonin syndrome—an urgent, potentially dangerous reaction. Do not mix them unless your prescriber specifically directs and monitors you.
What is the best time to take 5-HTP?
For sleep, take it 30–60 minutes before bed. For mood or appetite, add morning and mid‑afternoon doses. Avoid a late‑evening second dose if it leaves you groggy the next morning.
What side effects should I watch for with 5-HTP?
Nausea, heartburn, and drowsiness are most common, usually eased by taking with food and starting low. Stop and seek care for signs of serotonin overload: agitation, sweating, tremor, fast heart rate, or confusion—especially if on interacting drugs.
Is 5-HTP safe to take long term?
Short‑term use is generally well tolerated. For longer use, keep doses modest (100–300 mg/day), take breaks if possible, and review medications. Ongoing use in pregnancy or with bipolar disorder isn’t advised.
Can I combine 5-HTP and melatonin?
You can, but start low with one agent first. If needed, add a small melatonin dose (0.3–1 mg) with 5-HTP at bedtime. Higher combined doses increase next‑day grogginess and, with certain meds, risk serotonin issues.
Do I need blood tests before taking 5-HTP?
No specific test is required. If you’re concerned about conversion, checking Vitamin B6, Plasma can be useful. Routine serotonin blood tests don’t guide dosing and aren’t recommended for this purpose.
How to take it & ingredients
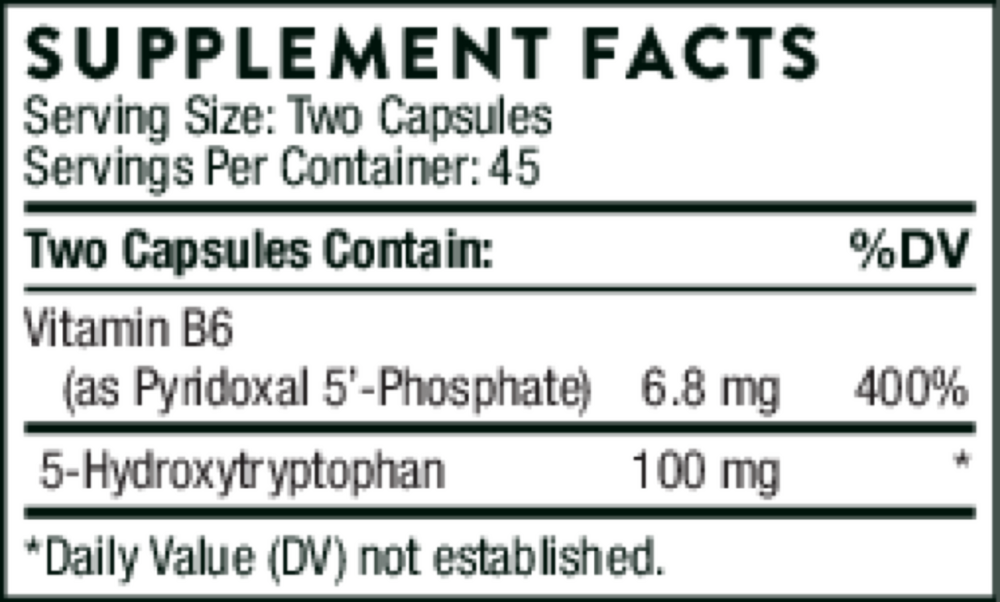
Suggested use: Take 1–2 capsules three times daily or as recommended by your health professional.
Active ingredients
2 capsules per serving · 45 servings
5-Hydroxytryptophan
100 mg
Vitamin B6
Pyridoxal 5'-Phosphate
Pyridoxal 5'-Phosphate
6.8 mg
Other ingredients: Hypromellose Capsule, Leucine, Microcrystalline Cellulose, Silicon Dioxide
Certifications
Benefits
Warnings