

Integrative Therapeutics
Active B-Complex by Integrative Therapeutics
60 capsules · 30-day supply
Comprehensive B Vitamin Support for Energy and Metabolism$XX.XX$18.99retail
Purchase option
21% below MSRP3rd-party tested for purity & potencyFree shipping $50+
Gluten Free·Soy Free·Dairy Free·Wheat Free·Artificial Color Free·Artificial Flavor Free
Integrative Therapeutics Active B-Complex overview
If your Homocysteine runs high or your Vitamin B12 or Folate markers are low, a methylated B complex is a practical fix. It’s also a fit for vegans and vegetarians, people on metformin or acid-suppressing drugs (both can lower B12), and heavy alcohol users. If fatigue, brain fog, or low mood track with a low-normal B12 or Folate, active forms often work better than standard folic acid and cyanocobalamin. This dose is repletion-leaning; long-term daily use is usually 1 capsule, not 2.
Methylfolate and methylcobalamin are the ready-to-use forms of folate and B12. They help recycle homocysteine (a byproduct that stresses blood vessels) back into methionine, which your body uses to add methyl groups (a simple chemical tag) that regulate DNA, neurotransmitters, and energy metabolism. Riboflavin and niacinamide feed mitochondrial enzymes that turn food into ATP, while P5P, the active B6, helps make serotonin and GABA, the brain’s calming signal. These changes show up on Homocysteine and Methylmalonic Acid within 4–8 weeks.
Take 1 capsule with breakfast. If your Homocysteine is high or your Methylmalonic Acid suggests low B12, use 2 capsules for 4 to 8 weeks, then retest and step down. Morning is best to avoid late-day alertness. It’s fine with or without food, but food reduces mild nausea. Expect bright yellow urine from riboflavin—that’s normal, not dehydration.
If you take methotrexate for cancer or autoimmune disease, ask your clinician before any folate; it can interfere with treatment plans. Levodopa without carbidopa can be inactivated by vitamin B6, so avoid this B complex in that scenario. Long-term high B6 can cause neuropathy; if you use 2 capsules (100 mg B6/day), keep it short and monitor symptoms. Pregnancy is better served by a prenatal with iodine, iron, and choline targets.
Frequently asked questions
How long does a B complex take to work?
Energy and mental clarity often improve within 1–2 weeks. Lab shifts take longer: Homocysteine and Methylmalonic Acid typically improve within 4–8 weeks. Retest after 6–8 weeks to gauge response and adjust the dose.
Will a B complex keep me awake?
It can if taken late. B vitamins participate in energy production, so take them in the morning. If you’re sensitive, avoid doses after 2 p.m. Insomnia isn’t common, but timing solves it for most people.
Does this B complex cause niacin flush?
No. It uses niacinamide, a non-flushing form of vitamin B3. You get the metabolic benefits without the warm, red flushing you can see with higher-dose niacin.
Is a methylated B complex better if I have an MTHFR variant?
Yes. Methylfolate bypasses the MTHFR enzyme step, which helps people who don’t convert folic acid efficiently. The practical measure is response: watch Homocysteine and how you feel over 4–8 weeks.
Can I take a B complex with metformin or a PPI?
Yes, and it’s often useful. Metformin and acid-suppressing drugs can lower B12 over time. A methylated B complex can help maintain levels, but still track Vitamin B12 and Methylmalonic Acid annually.
What labs should I check with a B complex?
Start with Vitamin B12, Folate, Homocysteine, and Methylmalonic Acid. If fatigue is a key symptom, include a CBC and Ferritin to rule out anemia and iron deficiency as separate issues.
Can B6 in this formula cause nerve issues?
High, long-term B6 can. Each capsule has 50 mg; stay at one daily for maintenance. If you use two daily short term, limit it to 4–8 weeks and step down. Report numbness or tingling promptly.
Why is my urine bright yellow after taking B complex?
That’s riboflavin (vitamin B2) being excreted. It’s harmless and expected. It doesn’t mean you’re dehydrated or that the B complex isn’t being used.
How to take it & ingredients
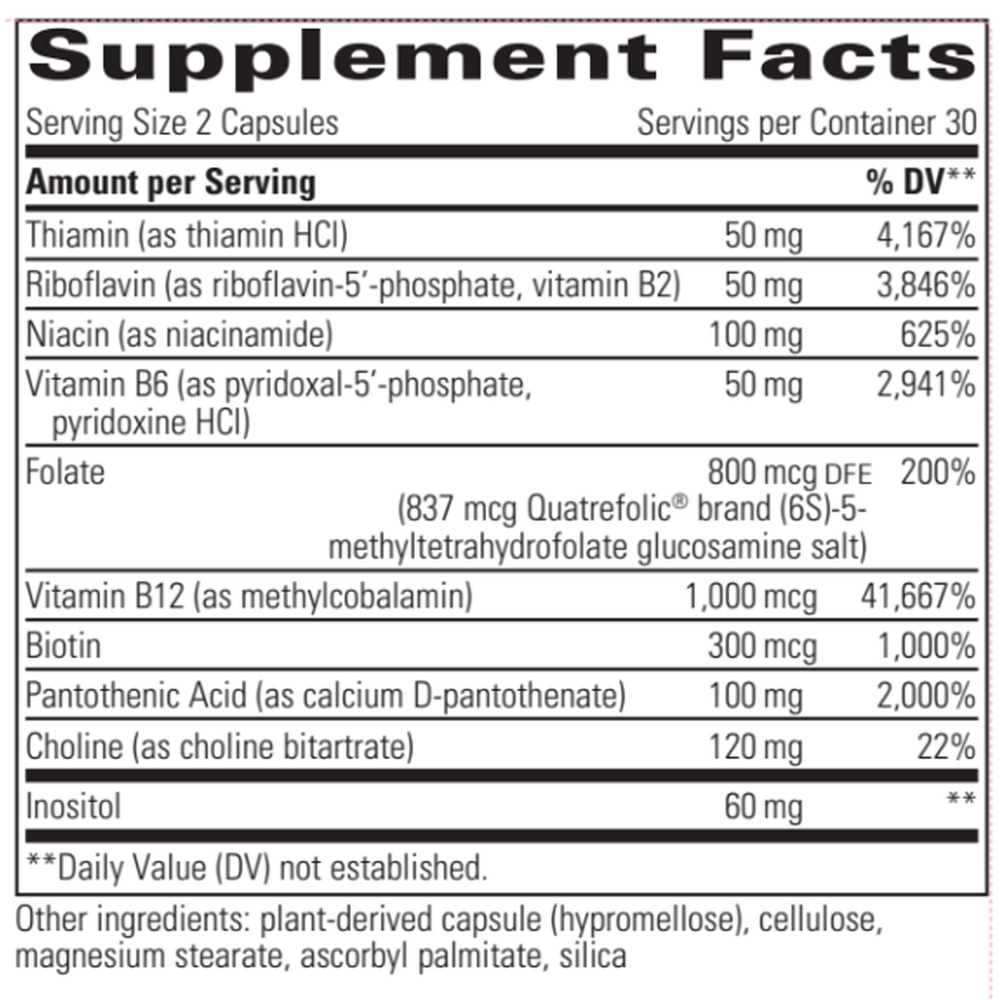
Suggested use: Adults take 1 to 2 capsules daily or as recommended by a healthcare professional.
Active ingredients
2 capsules per serving · 30 servings
Thiamin
Thiamin HCl
Thiamin HCl
50 mg
Riboflavin
Riboflavin 5 phosphate and Vitamin B2
Riboflavin 5 phosphate and Vitamin B2
50 mg
Niacin
Niacinamide
Niacinamide
100 mg
Vitamin B6
Pyridoxal 5 phosphate and Pyridoxine HCl
Pyridoxal 5 phosphate and Pyridoxine HCl
50 mg
Folate
Quatrefolic (6S)-5 methyltetrahydrofolate glucosamine salt
Quatrefolic (6S)-5 methyltetrahydrofolate glucosamine salt
800 mcg DFE, 837 mcg
Vitamin B12
Methylcobalamin
Methylcobalamin
1000 mcg
Biotin
300 mcg
Pantothenic Acid
Calcium D pantothenate
Calcium D pantothenate
100 mg
Choline
Choline bitartrate
Choline bitartrate
120 mg
Inositol
60 mg
Other ingredients: Plant derived capsule (hypromellose), Cellulose, Magnesium stearate, Ascorbyl palmitate, Silica
Certifications
Benefits
Warnings



