

Jarrow Formulas
B-12 & Folate Ultra Strength Cherry by Jarrow Formulas
60 chewables
Ultra Strength Support for Energy, Mood, and Cellular Health$47.99
Purchase options
Practitioner-grade brand3rd-party testedFree shipping $50+
Vegan·Vegetarian·Gluten Free·Soy Free·Dairy Free·Milk Free·
Jarrow Formulas B-12 & Folate Ultra Strength Cherry overview
If you’re looking for methylcobalamin 5000 mcg because your labs suggest low B12 status, this fits. It’s for vegans and vegetarians, long‑term metformin or acid‑reducing drug users, adults after bariatric surgery, and those with symptoms plus low or low‑normal Vitamin B12 or elevated Methylmalonic Acid (MMA) or Homocysteine. The included 5‑MTHF (the active folate form) helps if you have an MTHFR variant or a low RBC Folate. If your levels are healthy and you want maintenance, this dose is likely higher than you need.
Methylcobalamin (active B12) donates methyl groups, a simple chemical tag used in methylation, to convert homocysteine into methionine, which your body uses to make neurotransmitters and repair DNA. 5‑MTHF (active folate) feeds the same reaction, and because it bypasses the MTHFR enzyme step, it works even if that enzyme is sluggish. Pyridoxal‑5‑phosphate (P5P, active B6) supports the alternate pathway that clears homocysteine into cystathionine. Together, these forms tend to lower Homocysteine within 4 to 12 weeks and correct MMA and Vitamin B12 labs in true deficiency.
Let one cherry tablet dissolve in your mouth daily; buccal absorption helps if stomach or intrinsic factor is an issue. Morning is sensible since B12 can feel energizing. Take with or without food. This is a repletion‑level dose; once Vitamin B12, MMA, and Homocysteine normalize (often by 8–12 weeks), many people step down to a lower daily B12 and folate for maintenance. If you’re pregnant or planning, confirm your total folate from all sources with your clinician to avoid unnecessary stacking.
If you’re on methotrexate for cancer, do not add folate or 5‑MTHF unless your oncologist instructs it; it can counter the drug. Folate can also interact with trimethoprim or pyrimethamine, and high B6 can lessen levodopa’s effect if taken without carbidopa (this P5P dose is low, but caution still applies). Chloramphenicol can blunt the blood response to B12. Rarely, B12 triggers acne; spacing doses or stepping down usually solves it. Jarrow Formulas uses methylcobalamin and 5‑MTHF, which avoid cyanide‑based forms but the clinical cautions are the same.
How fast will I feel it? Energy changes are hit‑or‑miss, but lab shifts in Vitamin B12, MMA, and Homocysteine show up within 4–12 weeks. Can folate “mask” B12 deficiency? Large folate doses can hide anemia signs, which is why pairing with high‑dose B12 here is appropriate. Is methylcobalamin better than cyanocobalamin? It skips conversion steps and is well‑tolerated; both correct deficiency, but many clinicians prefer methyl forms when Homocysteine is high.
Frequently asked questions
Is 5000 mcg of B12 too much to take daily?
For deficiency or absorption issues, 5000 mcg is a common repletion dose and is considered safe because B12 has no established upper limit. Once Vitamin B12, MMA, and Homocysteine normalize, most people step down to a lower maintenance dose.
How long does methylcobalamin take to raise B12 levels?
Serum Vitamin B12 often rises within weeks, with clearer changes in Methylmalonic Acid and Homocysteine by 4–12 weeks. Recheck labs after 8–12 weeks to confirm response and adjust the dose.
Does methylfolate help if I have an MTHFR mutation?
Yes. 5‑MTHF is the active folate form and bypasses the MTHFR enzyme step. It’s useful when RBC Folate is low or Homocysteine is elevated despite adequate folic acid intake.
Should I take B12 and folate with food or on an empty stomach?
Either is fine. Letting the tablet dissolve in your mouth can improve uptake if stomach absorption is impaired. Morning dosing is preferred by many to avoid interfering with sleep.
Can this lower high homocysteine?
Often, yes. Methylcobalamin, 5‑MTHF, and P5P work on the pathways that recycle or clear homocysteine. Many see meaningful reductions within 4–12 weeks when levels were high to start.
Are there medications that interact with methylfolate or B12?
Cancer‑dose methotrexate, trimethoprim, and pyrimethamine interact with folate metabolism; use only under clinician guidance. Chloramphenicol can blunt B12’s blood response. High B6 can counter levodopa without carbidopa.
What side effects should I watch for?
B12 is usually well‑tolerated; occasional acne or restlessness can occur at high doses. Folate can cause mild nausea in some. If you feel overstimulated, move the dose earlier or reduce under guidance.
Do I still need a lower‑dose B12 after this?
Usually yes. After repletion and normalized labs, most people maintain with a lower daily B12 and folate. Your follow‑up Vitamin B12, MMA, and Homocysteine results should guide the maintenance plan.
How to take it & ingredients
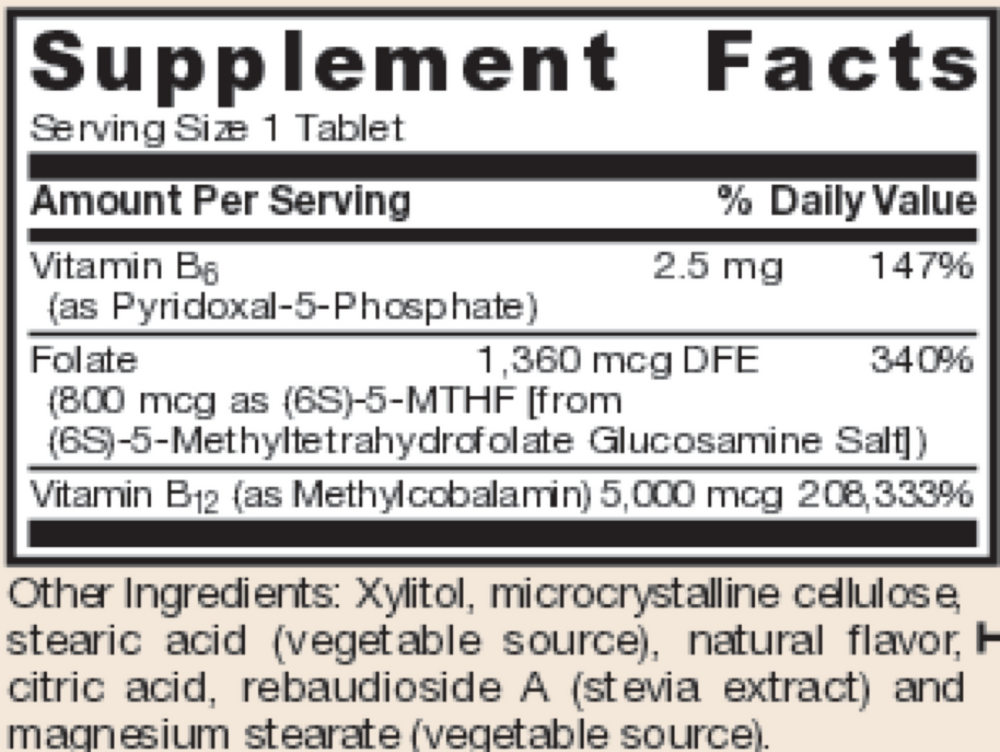
Suggested use: Dissolve in mouth or chew 1 tablet per day or as directed by your qualified healthcare professional.
Active ingredients
1 tablet per serving
Vitamin B6
Pyridoxal-5-Phosphate
Pyridoxal-5-Phosphate
2.5 mg
Folate
(6S)-5-MTHF [from Quatrefolic® (6S)-5-methyltetrahydrofolate glucosamine salt]
(6S)-5-MTHF [from Quatrefolic® (6S)-5-methyltetrahydrofolate glucosamine salt]
800 mcg
Vitamin B12
Methylcobalamin
Methylcobalamin
5000 mcg
Other ingredients: Xylitol, Cellulose, Stearic Acid (vegetable source), Natural Cherry Flavor, Citric Acid, Organic Rebiana (Stevia) Extract, Magnesium Stearate (vegetable source)
Certifications
Benefits
Warnings


