


Klaire Labs/SFI Health
Ther-Biotic Complete Probiotic 25 billion CFU (255 mg) by Klaire Labs/SFI Health
60 capsules · 60-day supply
A Balanced Probiotic Blend for Digestive and Immune Health$52.99retail
Add to cart for 21% off
This item is currently out of stockGet notified when this item is back in stock
21% below MSRP3rd-party tested for purity & potencyFree shipping $50+
Vegetarian·Gluten Free·Soy Free·Dairy Free·Egg Free·Tree Nut Free·
Klaire Labs/SFI Health Ther-Biotic Complete Probiotic overview
If you bloat after meals or feel gassy by evening, a multi‑strain probiotic is a reasonable first step. This 25 billion CFU blend fits people easing back from antibiotics, frequent travelers with loose stools, and those with irregularity. It’s a maintenance‑level dose for daily use. If your symptoms are severe, or your stool tests show high fecal calprotectin (an inflammation marker in stool) or low secretory IgA (the gut’s antibody), you’ll likely need a clinician‑guided plan beyond a general probiotic.
A broad probiotic mix of Lactobacillus and Bifidobacterium species competes with gas‑producing microbes, makes short‑chain fatty acids (small fats your gut bacteria produce from fiber that calm the colon), and strengthens tight junctions (the seals between intestinal cells). These microbes also nudge immune cells to raise secretory IgA (your gut’s first‑line antibody). In trials, multi‑strain probiotics cut antibiotic‑associated diarrhea by about one‑third to one‑half and can modestly lower hs-CRP (a blood marker of inflammation) in some responders over 4 to 8 weeks.
Take one capsule daily with food; a meal helps more bacteria survive stomach acid. If you’re sensitive to gas, start every other day for a week, then move to daily. On antibiotics, separate the probiotic by 2 to 3 hours. Expect changes in stool form within 1 to 2 weeks and bloating to settle, if it’s going to, within 4 to 8 weeks. The inulin base (a prebiotic fiber) can increase gas early; that usually fades as your microbiome adapts.
If you’re severely immunocompromised, have a central venous line, or are in the ICU, avoid live probiotics unless your care team directs otherwise. Recent severe pancreatitis is also a time to avoid them. Marked bloating from small intestinal bacterial overgrowth can worsen on broad probiotics; consider a targeted approach and breath testing (glucose or lactulose). If inulin triggers symptoms on a low-FODMAP plan, pick a probiotic without added prebiotic fiber. Pregnant and nursing adults generally tolerate probiotics, but discuss persistent symptoms with your clinician.
Frequently asked questions
Will this probiotic help with bloating?
Often, yes for meal‑related bloating, but not always. Multi‑strain probiotics can reduce gas and pressure over 4 to 8 weeks. If bloating is severe, progressive, or paired with weight loss, see a clinician to rule out small intestinal bacterial overgrowth or other causes.
How long does a probiotic take to work?
Bowel regularity changes are common within 1 to 2 weeks. Bloating, abdominal discomfort, and overall IBS‑type symptoms typically need 4 to 8 weeks. If there’s no benefit by 8 weeks, reconsider the diagnosis or switch to a different strain profile.
Can I take a probiotic with antibiotics?
Yes. Take the probiotic 2 to 3 hours away from each antibiotic dose. Starting on day one of antibiotics and continuing for at least a week after the course lowers the risk of antibiotic‑associated diarrhea in many people.
Do probiotics need refrigeration?
Store as the label directs. Many modern probiotics are shelf‑stable during shipping but last longer when kept cool and dry. Heat and humidity shorten shelf life; avoid bathroom cabinets and hot cars.
What side effects should I expect at first?
Mild gas, a fuller feeling, or looser stools can occur in the first week and usually settle as your microbiome adjusts. Persistent pain, fever, or blood in the stool is not normal—stop and seek care.
Is 25 billion CFU enough?
For daily maintenance and post‑antibiotic recovery, 25 billion CFU is a reasonable starting dose. Some people with stubborn IBS symptoms try higher CFU or strain‑specific products; dose matters less than choosing strains that fit your symptoms.
Is this probiotic safe in pregnancy or breastfeeding?
Generally yes for healthy adults, and it’s commonly used for regularity during pregnancy. If you have significant immune issues, a high‑risk pregnancy, or persistent GI symptoms, check with your obstetric clinician first.
Can probiotics raise nutrient absorption?
They can, modestly. By improving gut barrier function and producing short‑chain fatty acids, probiotics may aid absorption of minerals like magnesium and calcium. If your Vitamin B12 or iron is low, test and treat directly rather than relying on a probiotic alone.
How to take it & ingredients
Suggested use: Adults: 1 capsule daily with food or as directed by a healthcare professional. Children: As directed by a healthcare professional.
Active ingredients
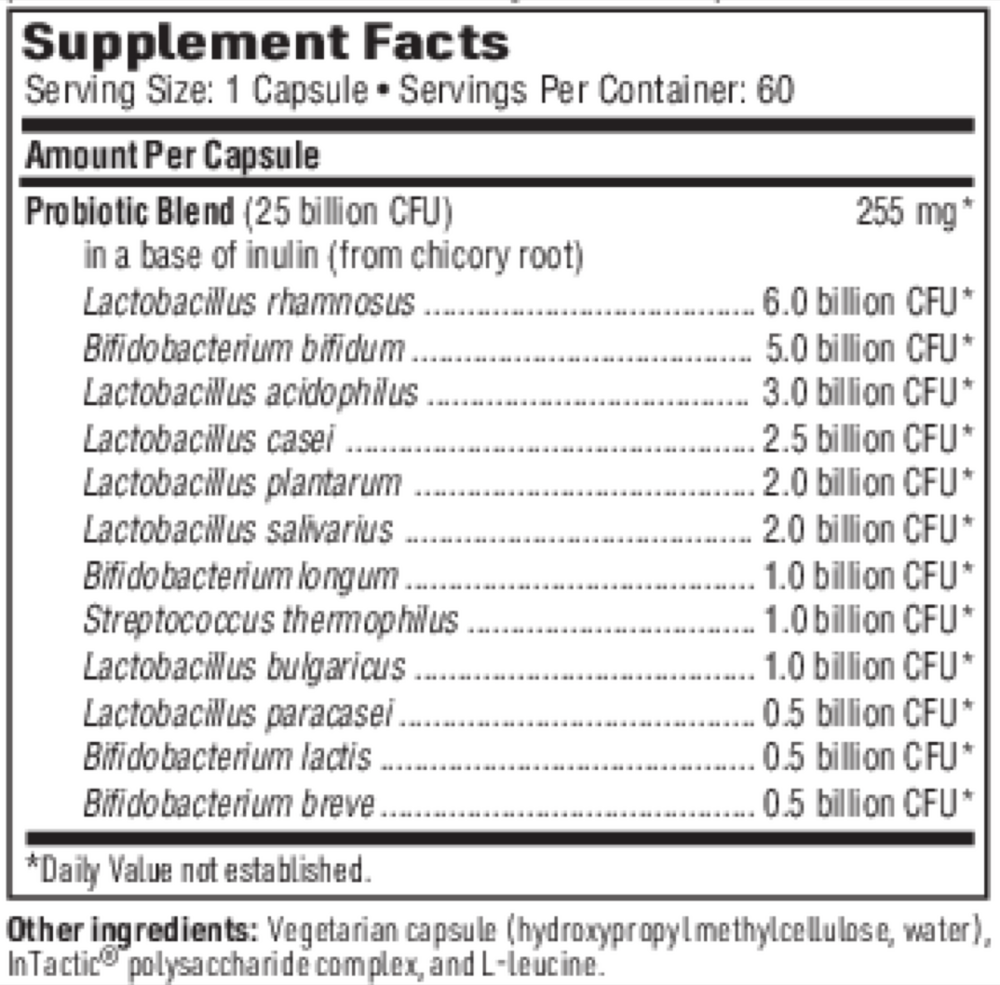
1 capsule per serving · 60 servings
▼
Probiotic Blend
25 billion CFU, 255 mg
Lactobacillus rhamnosus
6 billion CFU
Bifidobacterium bifidum
5 billion CFU
Lactobacillus acidophilus
3 billion CFU
Lactobacillus casei
2.5 billion CFU
Lactobacillus plantarum
2 billion CFU
Lactobacillus salivarius
2 billion CFU
Bifidobacterium longum
1 billion CFU
Streptococcus thermophilus
1 billion CFU
Lactobacillus bulgaricus
1 billion CFU
Lactobacillus paracasei
0.5 billion CFU
Bifidobacterium lactis
0.5 billion CFU
Bifidobacterium breve
0.5 billion CFU
Other ingredients: Hydroxypropyl methylcellulose, Water, InTactic® proprietary polysaccharide complex, L-leucine
Certifications
Benefits
Warnings