

Metagenics
Bone Builder Plus by Metagenics
90 capsules · 45-day supply
Essential Nutrients for Strong Bones and Overall Skeletal Health$XX.XX$39.99retail
This item is currently out of stockGet notified when this item is back in stock
20% below MSRP3rd-party tested for purity & potencyFree shipping $50+
Vegetarian·Gluten Free
Metagenics Bone Builder Plus overview
If you’re comparing calcium forms, microcrystalline hydroxyapatite (hydroxyapatite calcium) is a fit when bone density is a real concern, not just general “bone health.” It suits post‑menopausal women, men over 50 with low dietary calcium, and anyone with a DXA scan showing bone loss. It also helps if your Vitamin D, 25-Hydroxy is in the lower end of normal and you want a maintenance 2,000 IU of vitamin D3 built in. If you’re on long‑term steroids, have a small frame, or avoid dairy, this is a practical way to cover the base minerals.
Hydroxyapatite provides calcium and phosphorus in the same ratio found in human bone, along with bone matrix proteins like collagen. That combination feeds both the mineral and the scaffold your skeleton uses, which is why some trials show better bone density retention than plain calcium carbonate. Vitamin D3 (cholecalciferol) raises calcium absorption from the gut and lowers parathyroid hormone, the signal that pulls calcium from bone, so you lose less during normal bone turnover. Track response with DXA and, if available, bone turnover markers like CTX (a breakdown marker) or P1NP (a formation marker).
Take two capsules once daily with food for better absorption and fewer GI symptoms. The 420 mg of calcium here is a maintenance slice of a typical adult daily goal; most people reach their target by combining this with diet. If you need more than 500–600 mg from supplements, split doses 6–12 hours apart. Separate calcium by 2–4 hours from thyroid medication, high‑dose iron, tetracycline or fluoroquinolone antibiotics, and morning alendronate.
Skip this or use only with clinician guidance if you’ve had high blood calcium, recurrent calcium‑oxalate kidney stones, sarcoidosis, or parathyroid disease. Thiazide diuretics (like hydrochlorothiazide) raise blood calcium; combining them with calcium supplements needs monitoring. If you use a proton‑pump inhibitor for reflux, hydroxyapatite tends to be easier to absorb than carbonate, but spacing doses with other meds still matters. This formula is bovine‑sourced, so it’s not vegan and should be avoided with beef allergy.
Expect measurable changes in bone density on DXA after 6–12 months, not weeks. If constipation shows up, increase fluids, add magnesium at night, or split the dose. hs-CRP (a general inflammation marker) isn’t how we track bone response; focus on DXA and, when available, CTX or P1NP. Keep vitamin K intake steady from food if you’re on warfarin—don’t add K supplements without approval.
Frequently asked questions
Is microcrystalline hydroxyapatite better than calcium citrate or carbonate?
For bone density specifically, hydroxyapatite has evidence of equal or better retention versus carbonate in some trials, likely due to the bone‑matrix components. Citrate is gentler on the stomach. If your DXA shows loss, hydroxyapatite is a strong first pick; if you’re sensitive to calcium, citrate can be easier.
How long does hydroxyapatite calcium take to work?
Bone changes slowly. Plan on 6–12 months before a DXA scan can show a difference. Day‑to‑day you won’t feel anything; tracking relies on DXA and, if available, bone turnover labs like CTX (resorption) or P1NP (formation).
Can I take this calcium with magnesium or vitamin K2?
Yes, magnesium and vitamin K2 are commonly paired with calcium for bone programs. Magnesium can reduce constipation. If you take warfarin, avoid adding K2 without your prescriber’s approval, as it interacts with dosing.
Does hydroxyapatite calcium cause constipation or stomach upset?
It can, though many people tolerate hydroxyapatite better than carbonate. Take it with meals, split larger calcium intakes into two doses, hydrate, and consider evening magnesium if constipation appears.
Is 2,000 IU of vitamin D3 too much to take daily?
For most adults, 2,000 IU is a common maintenance dose. The right dose depends on your Vitamin D, 25-Hydroxy level, skin tone, body weight, and sun exposure. Re‑check your level after 8–12 weeks and adjust with your clinician.
Can I take hydroxyapatite calcium with thyroid medication?
Yes, but separate them. Calcium binds levothyroxine in the gut and blocks absorption. Take thyroid medication on an empty stomach and wait at least 2–4 hours before taking calcium.
Is microcrystalline hydroxyapatite vegan or dairy‑free?
It’s bovine‑sourced (from beef bone), so it’s not vegan or vegetarian. It doesn’t contain milk sugar, but those with beef allergy should avoid it. If you need a vegan option, consider calcium citrate or algae‑derived calcium.
Who should avoid calcium supplements altogether?
People with high blood calcium, active kidney stones, sarcoidosis, or parathyroid disorders should avoid unsupervised calcium. Certain diuretics and high vitamin D states also need caution. Work with a clinician before adding calcium.
How to take it & ingredients
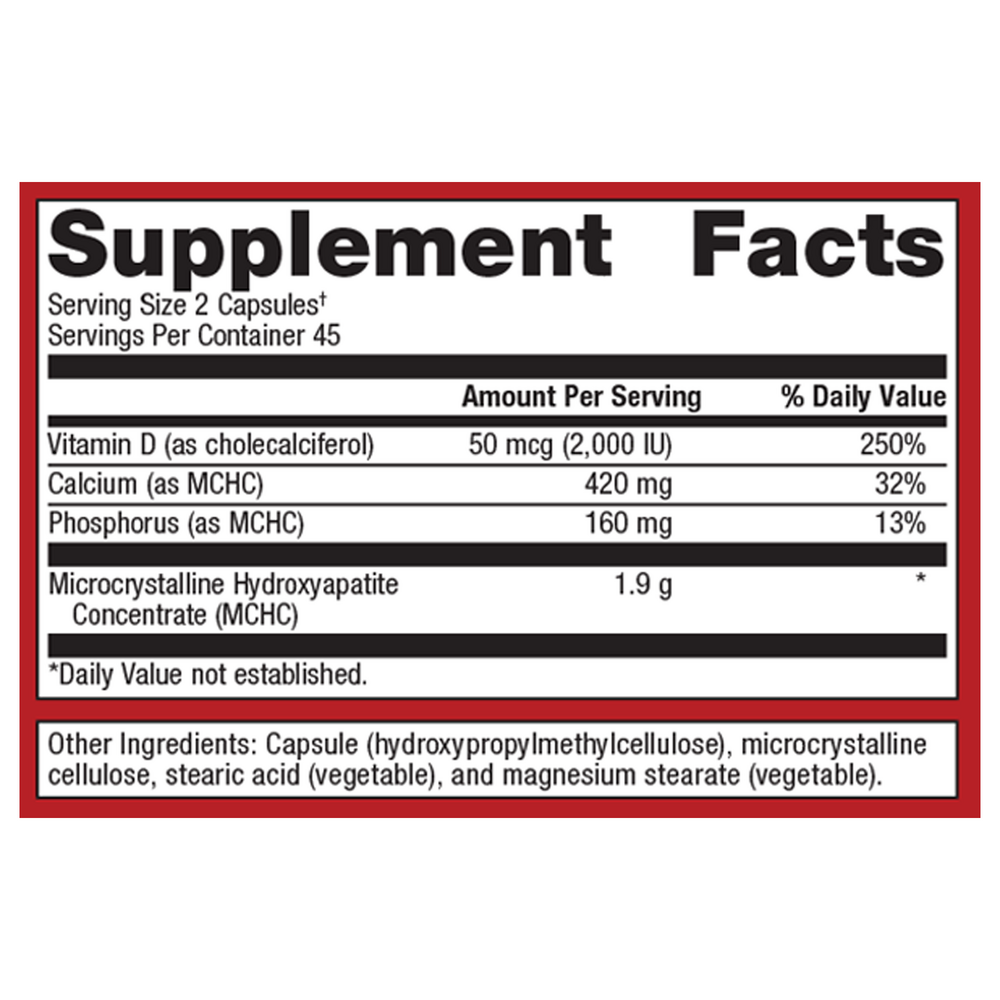
Suggested use: Take 2 capsules once daily. Do not exceed the recommended dosage unless directed by your healthcare practitioner.
Active ingredients
2 capsules per serving · 45 servings
Vitamin D3
Cholecalciferol
Cholecalciferol
2000 IU, 50 mcg
Calcium
Microcrystalline hydroxyapatite concentrate (MCHC)
Microcrystalline hydroxyapatite concentrate (MCHC)
420 mg
Phosphorus
Microcrystalline hydroxyapatite concentrate (MCHC)
Microcrystalline hydroxyapatite concentrate (MCHC)
160 mg
Microcrystalline Hydroxyapatite Concentrate (MCHC)
1900 mg
Other ingredients: Hydroxypropylmethylcellulose (capsule), Microcrystalline cellulose, Stearic acid (vegetable), Magnesium stearate (vegetable)
Certifications
Benefits
Warnings