


Microbiome Labs
MegaSporeBiotic 4 billion CFU (295 mg) by Microbiome Labs
180 capsules · 90-day supply
Advanced Probiotic Support for Gut Health and Balance$168.99retail
Add to cart for 20% off
This item is currently out of stockGet notified when this item is back in stock
20% below MSRP3rd-party tested for purity & potencyFree shipping $50+
Soy Free·Salt Free·Wheat Free·Sugar Free·Organic·Artificial Color Free·
Microbiome Labs MegaSporeBiotic overview
If you’ve tried lactobacillus/bifido blends and still deal with bloating or irregularity, a spore-based probiotic is a logical next step. These Bacillus strains tolerate stomach acid and reach the intestines alive, which matters if your Comprehensive Stool Analysis shows low diversity or if your Omega-3 Index and hs-CRP (a blood marker of inflammation) suggest low-grade inflammation tied to the gut. Travelers, frequent antibiotic users, and people with loose stools after meals also tend to do well.
Bacillus spores germinate in the small intestine, then temporarily colonize and crowd out gas-producing species. They produce antimicrobial peptides (natural antibiotics made by bacteria), nudge beneficial microbes to make more butyrate (a short-chain fatty acid that fuels the gut lining), and tighten the gut barrier. In small trials with this strain mix, markers tied to leakiness like zonulin (a protein that regulates gut junctions) and LPS-binding protein (a proxy for bacterial endotoxin exposure) improved within 4 to 12 weeks, with some reduction in hs-CRP in responders.
Start low with food: 1/2 to 1 capsule daily for a week, then increase toward 2 capsules daily as tolerated. Gas or stool changes in the first 1 to 2 weeks usually reflect a microbiome shift—if uncomfortable, drop back for a few days, then re-titrate. Take with a meal for consistency. If you’re on antibiotics, separate by at least 2 to 3 hours. Expect bowel-pattern changes in 1 to 2 weeks and barrier or inflammation shifts in 4 to 12 weeks.
Avoid probiotics if you’re severely immunocompromised, have a central venous catheter, are immediately post–organ transplant, or are in the ICU unless your clinician approves. Use caution if you have significant small intestinal bacterial overgrowth (SIBO, bacterial overgrowth in the small bowel): symptoms can flare before settling. Pregnancy and breastfeeding: data are limited, so discuss with your obstetric clinician. Stop and seek care for fever, persistent severe abdominal pain, or blood in stool.
Frequently asked questions
Do spore-based probiotics need refrigeration?
No. Bacillus spores are naturally heat-stable and shelf-stable at room temperature. Keep the bottle dry and closed. Avoid storing in a hot car or humid bathroom to maintain potency through the labeled date.
How long until a spore probiotic helps bloating?
Bloating and stool consistency often improve within 1 to 2 weeks. Gut barrier and inflammation markers like zonulin or hs-CRP typically need 4 to 12 weeks. If nothing changes by week 6, reassess dose, diet, and whether a different tool fits better.
Can I take a spore probiotic with antibiotics?
Yes, but separate doses by 2 to 3 hours. Many Bacillus strains tolerate some antibiotics, yet spacing helps. Continue for at least 2 to 4 weeks after finishing antibiotics to stabilize the microbiome.
Can I open the capsule into food?
Yes. You can open it and sprinkle the contents into a cool, soft food. Avoid hot liquids that could damage viability. Start with a small amount if you’re sensitive.
What side effects should I expect?
Temporary gas, cramping, or looser stools are the most common in the first 1 to 2 weeks. They usually settle as your microbiome adjusts. If symptoms are intense, reduce the dose, take with meals, or pause and restart lower.
Is a spore-based probiotic safe in pregnancy?
Safety data in pregnancy are limited. Many clinicians are comfortable with probiotics, but choices are individualized. Discuss with your obstetric clinician before starting, especially if you have complications or take prescription meds.
Can I take a spore probiotic long term?
Yes. These strains transiently colonize and are commonly used daily. Many people stay on a maintenance dose after 8 to 12 weeks. Periodic breaks are reasonable; use your symptoms and stool pattern to guide.
How to take it & ingredients
Suggested use: Start with 1/2 to 1 capsule with food and gradually increase to 2 capsules daily. Reduce dose if side effects occur.
Active ingredients
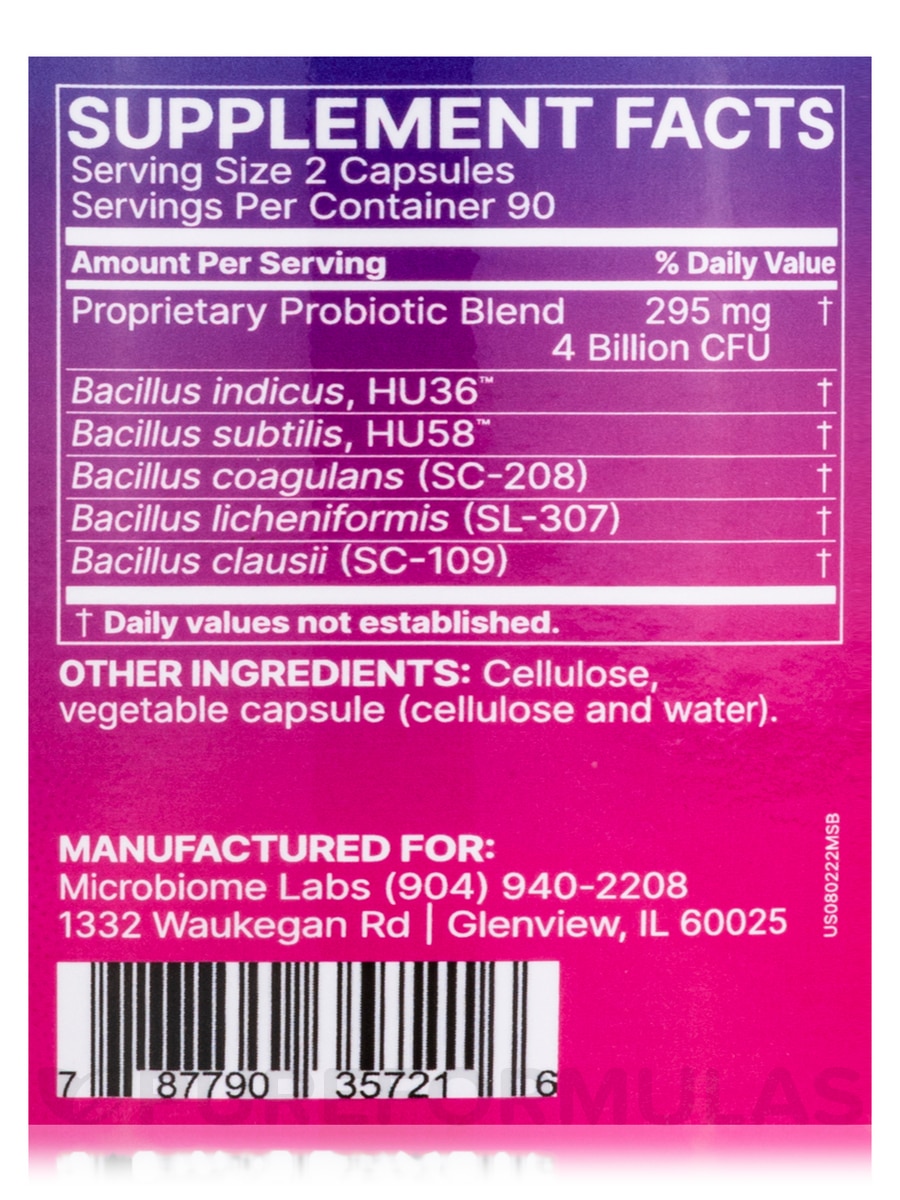
2 capsules per serving · 90 servings
▼
Proprietary Probiotic Blend
4 billion CFU, 295 mg
Bacillus indicus HU36
-
Bacillus subtilis HU58
-
Bacillus coagulans (SC-208)
-
Bacillus licheniformis (SL-307)
-
Bacillus clausii (SC-109)
-
Other ingredients: Cellulose, Vegetable capsule (cellulose, water)
Certifications
Benefits
Warnings