

Ortho Molecular Products
SBI Protect® Powder 2.5 g by Ortho Molecular Products
150 grams · 60-day supply
Support Your Immune System with Serum-Derived Immunoglobulins$158.79retail
Add to cart for 10% off
Purchase option
10% below MSRP3rd-party tested for purity & potencyFree shipping $50+
Gluten Free·Artificial Color Free·Artificial Flavor Free
Ortho Molecular Products SBI Protect® Powder overview
Frequent loose stools after antibiotics or travel, irritable bowel syndrome with diarrhea, and post-infectious gut upset are where bovine immunoglobulin powder earns its keep. If your stool testing shows elevated fecal calprotectin (a marker of gut inflammation) or low secretory IgA (the antibody your gut secretes into the lumen), this is a targeted option. The twice-daily 2.5 g scoop (5 g/day) is a clinically used dose; expect steadier stools within 2 to 4 weeks, with fuller symptom settling by 4 to 8 weeks.
These concentrated IgG antibodies are not systemically absorbed; they act inside the intestines. They bind bacterial fragments like LPS (endotoxin from gram‑negative bacteria), viral particles, and food antigens, which keeps them from triggering immune cells and irritating the lining. By neutralizing those triggers, stool frequency and urgency often drop, hs-CRP (a blood inflammation marker) may improve in responders, and barrier function can normalize, which you’ll feel as less bloating and more formed stools.
Mix one scoop in cool or room‑temperature liquid twice daily. Hot liquids can denature proteins, so keep it below coffee/tea temperatures. Take with or without food. Because it can bind substances in the gut, separate from medications and iron by 2 hours. If you’re sensitive, start with one scoop daily for a week, then increase. Maintain 5 g/day during active symptoms; some step down to 2.5 g/day once stable.
Avoid if you have a confirmed allergy to beef products or alpha‑gal syndrome (red‑meat allergy). It is dairy‑free, but anyone with severe milk or serum protein reactions should discuss with a clinician first. Not enough data for pregnancy or breastfeeding; get medical guidance. If you’re on complex biologic or immunosuppressive therapy, coordinate timing with your prescriber to avoid unintended binding in the gut.
Frequently asked questions
What is bovine immunoglobulin powder and what is it used for?
It’s a concentrated IgG protein from bovine serum that stays in the gut and binds microbial toxins and antigens. Clinically it’s used to calm loose stools, urgency, and post-infectious irritation, and to support a healthier gut barrier.
How long does bovine immunoglobulin take to work?
Stool consistency and urgency often improve within 2 to 4 weeks at 5 g/day. More stubborn cases may take 4 to 8 weeks. If nothing changes by 8 weeks, revisit dose, adherence, and other drivers with your clinician.
Can I take immunoglobulin powder with probiotics or medications?
Yes, but separate by about 2 hours. These antibodies can bind substances in the gut and could reduce the effect of oral medications, iron, or probiotics if taken together.
Is bovine immunoglobulin dairy-free and safe for lactose intolerance?
It’s derived from serum, not milk, so it’s lactose-free and casein-free. However, if you have beef allergy or alpha-gal syndrome, avoid it and discuss alternatives with your clinician.
Will it show up in my blood or affect antibodies on lab tests?
No. It acts locally in the intestines and isn’t meaningfully absorbed intact, so it doesn’t alter your blood immunoglobulin levels. Its effects show up in symptoms and sometimes in fecal calprotectin or secretory IgA.
Are there side effects or interactions to watch for?
Most tolerate it well. Mild constipation, gas, or fullness can occur, especially at higher doses; reduce and titrate up. Space it 2 hours from medications and iron to avoid binding in the gut.
Can I use it long term?
Many patients use it for several months, then taper once stools and triggers stabilize. Long-term use appears safe in studies, but periodic reassessment with stool markers or symptoms is sensible.
Does it help with elevated fecal calprotectin?
In responders, calming luminal triggers can lower fecal calprotectin over weeks to months. If your level stays high despite symptom gains, your clinician should look for other sources of inflammation.
How to take it & ingredients
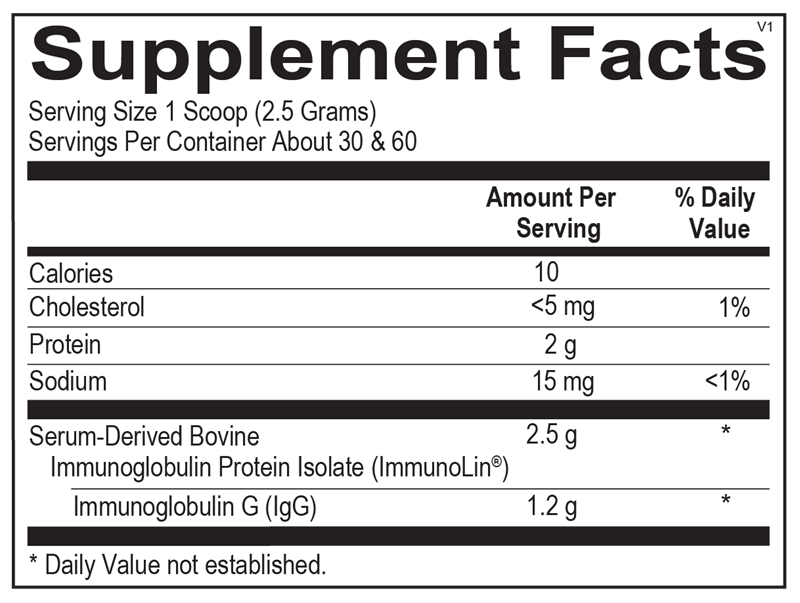
Suggested use: Mix 1 scoop (2.5 grams) with 4 ounces of water or your beverage of choice twice daily or as recommended by your health care professional. Stir until dissolved and consume immediately.
Active ingredients
1 scoop = 2.5 grams per serving · 60 servings
▼
Serum-Derived Bovine Immunoglobulin Concentrate
ImmunoLin®
ImmunoLin®
2.5 g
Immunoglobulin G
1.2 g
Certifications
Benefits
Warnings