

Pure Encapsulations
B12 Folate by Pure Encapsulations
60 capsules · 60-day supply
Essential B Vitamins for Energy, Mood, and Cellular Health$XX.XX$22.50retail
Purchase option
20% below MSRP3rd-party tested for purity & potencyFree shipping $50+
Vegan·Vegetarian·Gluten Free·Egg Free·Preservative Free·Peanut Free·
Pure Encapsulations B12 Folate overview
If you’re looking for a B12 and folate supplement because your labs show low Vitamin B12, lower-range Folate, or elevated Homocysteine (an amino acid tied to cardiovascular and brain aging), this pairing fits. Vegans and vegetarians, long‑term metformin or acid-suppressor users, and people with the MTHFR C677T variant often need active forms. It’s also useful if your Methylmalonic Acid (a B12 status marker) is high or your MCV (red blood cell size) is up. For pregnancy, use a dedicated prenatal instead.
This formula uses methylcobalamin (the methyl form of B12) and L‑5‑methyltetrahydrofolate, or L‑5‑MTHF (the bioactive folate your cells actually use). Together they recycle homocysteine back to methionine, a step central to methylation (the on/off tagging system for DNA and neurotransmitters). That underpins steady red blood cell production and supports neurotransmitter synthesis for mood and focus. Evidence for mood lift exists in some patients, but effects are modest and depend on baseline deficiency.
Take 1 capsule with a meal, once or twice daily as Pure Encapsulations suggests. If you’re sensitive to stimulation, take earlier in the day—methyl forms can feel energizing. Recheck Homocysteine, Vitamin B12, Folate, and Methylmalonic Acid within 8–12 weeks to judge response. If you have proven B12 malabsorption or pernicious anemia, oral capsules may be inadequate; injections or high-dose sublingual strategies are usually needed under clinician care.
Folate at high doses can mask the blood changes of B12 deficiency while nerve injury progresses, which is why pairing folate with B12 is prudent. Methotrexate for cancer is a red flag—don’t add L‑5‑MTHF without your oncologist. For autoimmune methotrexate, clinicians often use folate, but coordinate dosing. Anticonvulsants like valproate or carbamazepine interact with folate pathways—medical guidance advised. Metformin, PPIs, and H2 blockers lower B12 absorption, making this combo more relevant.
If you’ve had agitation, insomnia, or anxiety on high-dose methylfolate before, start low and titrate or consider folinic acid (a gentler folate form) with B12 supervision. Active cancer care, history of Leber hereditary optic neuropathy (a rare B12 issue), or unexplained anemia with neurologic symptoms warrant clinician evaluation before self‑supplementing. Planning pregnancy? Use a prenatal that includes L‑5‑MTHF or folic acid plus iodine, choline, and iron, rather than piecing together singles.
Homocysteine typically falls within 4–12 weeks if your baseline was high. Energy changes, if you notice them, usually appear in 1–2 weeks once B12 status improves. If your Vitamin B12 is low but Methylmalonic Acid is normal, investigate other causes of fatigue; more B12 isn’t always better. If your labs are normal and you eat animal foods regularly, routine high-dose B12 is unlikely to add benefit.
Frequently asked questions
Is methylfolate better than folic acid?
For many, both raise folate status. L‑5‑MTHF bypasses common MTHFR gene bottlenecks, so it’s preferred if you don’t process folic acid well or have elevated homocysteine. It also avoids unmetabolized folic acid in the blood. Clinically, the best choice hinges on your labs and tolerance.
How long does B12 and methylfolate take to lower homocysteine?
Expect changes within 4–12 weeks. Recheck Homocysteine along with Vitamin B12, Folate, and Methylmalonic Acid to confirm response. If homocysteine remains high, add riboflavin (B2) and vitamin B6, address hypothyroidism, kidney issues, or high alcohol intake, and review protein intake.
Can methylfolate cause anxiety or insomnia?
It can in sensitive people, especially at higher doses. Start with one capsule daily, take it earlier in the day, and consider reducing frequency. If symptoms persist, switch to folinic acid or use lower-dose combinations under guidance while you retest labs.
Does folate hide B12 deficiency?
High folate can correct anemia while B12‑related nerve damage continues. That’s why pairing folate with B12 is safer, and why testing Vitamin B12 and Methylmalonic Acid matters before and during folate use, especially if you have neurologic symptoms.
What’s the best time of day to take B12 and folate?
Take with food, ideally in the morning or at lunch. Methylcobalamin and methylfolate can feel energizing, so avoid late-evening doses if you’re prone to insomnia. Consistency matters more than clock time for homocysteine lowering.
Is this enough for vegans to cover B12 needs?
Often yes as maintenance, since it includes methylcobalamin. Confirm with Vitamin B12 and Methylmalonic Acid after 8–12 weeks. If absorption is impaired or levels remain low, higher-dose or sublingual B12, or injections, may be needed.
Can I take methylfolate and B12 with antidepressants?
Often, yes—and L‑methylfolate is sometimes used alongside SSRIs. Still, review with your prescriber, especially if you take bupropion or have bipolar spectrum conditions, and monitor for activation (restlessness, insomnia) when starting.
How to take it & ingredients
Suggested use: Take 1 capsule, 1-2 times daily, with meals.
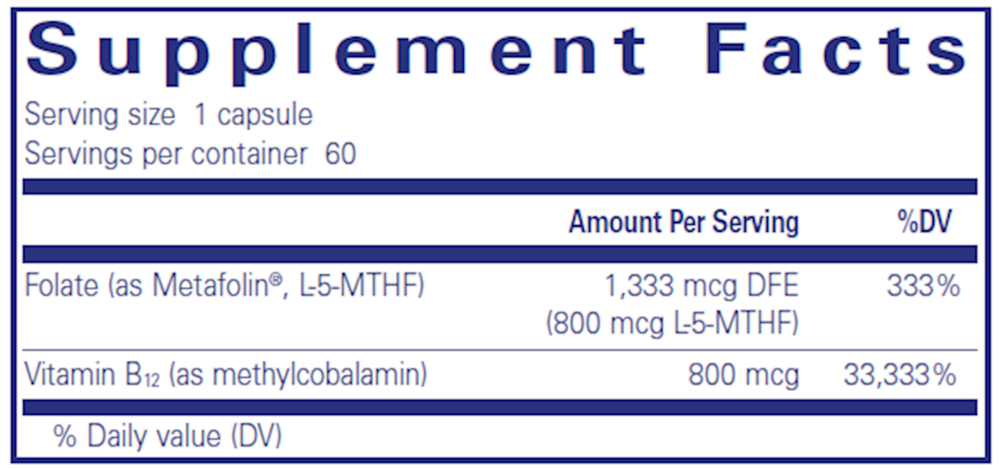
Active ingredients
1 capsule per serving · 60 servings
Folate
Metafolin®, L-5-methyltetrahydrofolate (L-5-MTHF)
Metafolin®, L-5-methyltetrahydrofolate (L-5-MTHF)
800 mcg
Vitamin B12
Methylcobalamin
Methylcobalamin
800 mcg
Other ingredients: Hypoallergenic plant fiber (cellulose), Ascorbyl palmitate, Vegetarian capsule (cellulose, water)
Certifications
Benefits
Warnings


