


Thorne
B-Complex #12 by Thorne
60 capsules · 60-day supply
Comprehensive B Vitamin Support for Energy and Metabolism$26.00retail
Add to cart for 19% off
Purchase option
19% below MSRP3rd-party tested for purity & potencyFree shipping $50+
Vegan·Vegetarian·Gluten Free·Soy Free·Dairy Free·Egg Free·
Thorne B-Complex #12 overview
If you’re looking for a methylated B complex to address low energy, brain fog, or a high Homocysteine (an amino acid linked to vascular risk), this formulation fits. It’s targeted for people with low or low‑normal Vitamin B12, those with MTHFR variants who don’t use folic acid well, vegans or metformin users with borderline B12, and anyone whose Methylmalonic Acid (a functional B12 marker) runs high. It’s also practical if you want a single B‑complex to cover biotin, choline, and higher‑potency B1, B2, B3, B5, and B6.
This B‑complex uses methylcobalamin (the active B12 your cells use) and L‑5‑MTHF (methylfolate, the ready‑to‑use folate) so your body doesn’t have to convert them. Together they drive methylation, the body’s carbon‑donation system for turning genes on and off and processing hormones and toxins, which is why they lower Homocysteine in responders. Higher‑potency thiamin, riboflavin, niacinamide, and pantothenate help enzymes turn carbs and fats into ATP, your cell’s energy currency. Vitamin B6 here supports neurotransmitter building for mood and focus, while niacinamide delivers niacin benefits without the flushing.
Start with one capsule in the morning with food; B‑vitamins can feel stimulating if taken late. If you’re under‑methylated with elevated Homocysteine, moving to twice daily often helps, and some use three daily short‑term. Expect steadier energy within 1–2 weeks, with Homocysteine shifts typically showing up on labs in 4–8 weeks. If you already take another multivitamin with B6 or folate, avoid doubling up—this B‑complex is a full‑strength dose.
Check Vitamin B12 and Methylmalonic Acid before long‑term folate if you’re older or on metformin or a proton‑pump inhibitor; folate can correct anemia signs while B12‑related nerve issues continue. Coordinate methylfolate with methotrexate therapy, anti‑seizure drugs, or active cancer care. If you combine multiple supplements, keep total daily vitamin B6 under high intakes, as very large chronic doses can cause nerve symptoms. Thorne’s B‑complex uses niacinamide, which rarely affects liver labs at standard doses.
Will this help immediately? Mental clarity often improves in days, but lab changes like Homocysteine take weeks. What’s different about methylfolate versus folic acid? Methylfolate is the end‑form the body uses directly, useful if you don’t convert folic acid efficiently. Why is my urine bright yellow? That’s excess riboflavin being excreted—harmless.
Frequently asked questions
How long does a B-complex take to work for energy?
Most people notice steadier energy and focus within 3–14 days. If you’re tracking Homocysteine or Vitamin B12, recheck labs after 4–8 weeks to see biochemical changes.
Is a methylated B complex better if I have an MTHFR variant?
Yes. Using L‑5‑MTHF (methylfolate) and methylcobalamin bypasses the conversion steps that MTHFR variants slow, and often lowers Homocysteine more reliably than folic acid.
Can I take this B-complex at night?
You can, but B‑vitamins sometimes feel stimulating. Morning or midday with food is preferred. If you’re sensitive, avoid dosing after 3 p.m.
Does B-complex cause niacin flushing?
Not this one. It uses niacinamide, a non‑flushing form of vitamin B3, so you get metabolic benefits without the warm, red flush from nicotinic acid.
What labs should I check with a B-complex?
Useful markers include Vitamin B12, Methylmalonic Acid, Homocysteine, and Folate. If you’re treating deficiency or symptoms, recheck after 4–8 weeks.
Is this B-complex safe in pregnancy?
At these amounts, methylfolate and methylcobalamin are pregnancy‑compatible. Still, review your full prenatal stack with your clinician to avoid duplicating B‑vitamins.
Can B6 in a B-complex cause neuropathy?
Only at high chronic intakes, typically far above this dose. Keep total daily B6 from all supplements moderate and discuss long‑term use if you have nerve symptoms.
Will metformin or PPIs affect my need for B12?
Yes. Metformin and proton‑pump inhibitors can lower B12 status over time. This B‑complex supplies methylcobalamin, but checking Vitamin B12 and Methylmalonic Acid is smart.
How to take it & ingredients
Suggested use: Take 1 capsule one to three times daily or as recommended by your health professional.
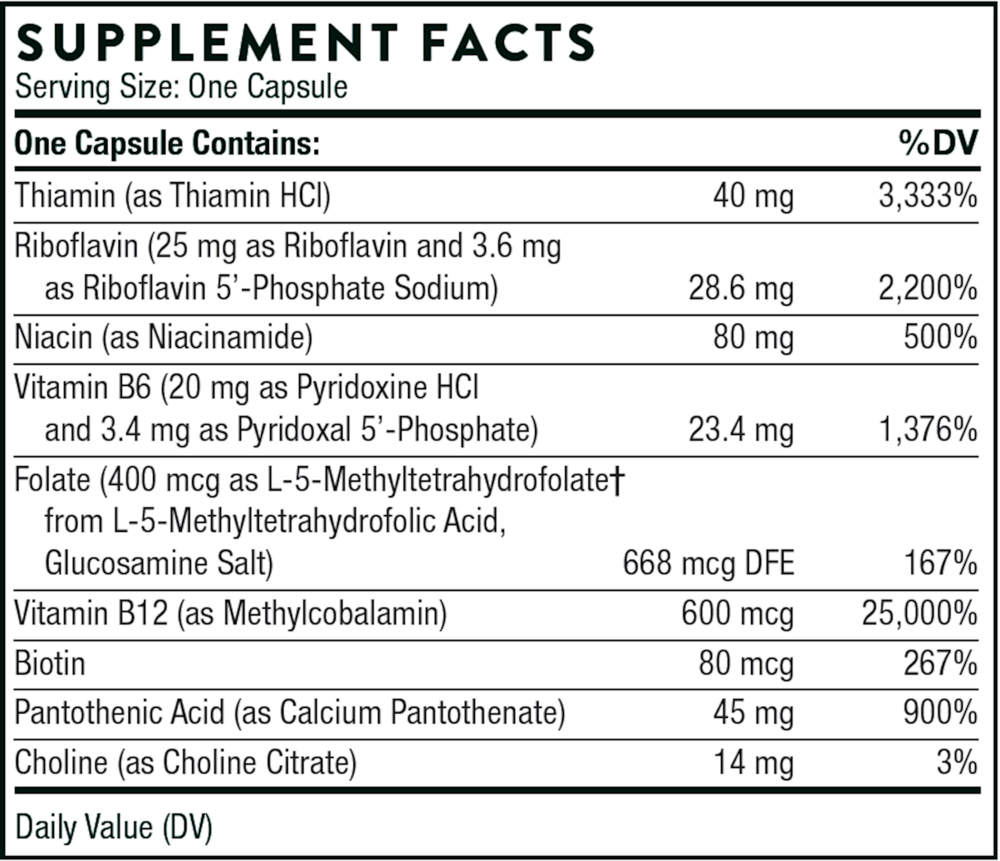
Active ingredients
1 capsule per serving · 60 servings
Biotin
80 mcg
Choline
Choline Citrate
Choline Citrate
14 mg
Folate
L-5-Methyltetrahydrofolate from L-5-Methyltetrahydrofolic, Glucosamine Salt
L-5-Methyltetrahydrofolate from L-5-Methyltetrahydrofolic, Glucosamine Salt
400 mcg
Thiamin
Thiamin HCI
Thiamin HCI
40 mg
Vitamin B12
Methylcobalamin
Methylcobalamin
600 mcg
▼
Riboflavin
28.6 mg
Riboflavin
Riboflavin 5'-Phosphate Sodium
Riboflavin 5'-Phosphate Sodium
3.6 mg
Riboflavin
Riboflavin
Riboflavin
25 mg
Niacin
Niacinamide
Niacinamide
80 mg
Pantothenic Acid
Calcium Pantothenate
Calcium Pantothenate
45 mg
▼
Vitamin B6
23.4 mg
Vitamin B6
Pyridoxine HCL
Pyridoxine HCL
20 mg
Vitamin B6
Pyridoxal 5'-Phosphate
Pyridoxal 5'-Phosphate
3.4 mg
Other ingredients: Calcium Laurate, Hypromellose Capsule, Microcrystalline Cellulose, Silicon Dioxide
Certifications
Benefits
Warnings