


Thorne
Basic B Complex by Thorne
60 capsules · 60-day supply
Comprehensive B Vitamin Support for Energy and Metabolism$27.00retail
Add to cart for 19% off
Purchase option
19% below MSRP3rd-party tested for purity & potencyFree shipping $50+
Gluten Free·Soy Free·Dairy Free·Milk Free
Thorne Basic B Complex overview
If you’re searching for the best B complex for energy, this fits adults who feel run-down despite decent sleep and whose labs hint at low B status. Useful flags include a low-normal Vitamin B12, elevated Methylmalonic Acid (MMA, a functional B12 marker), higher Homocysteine (an amino acid that rises when folate or B12 are low), or low RBC Folate. It’s also a practical pick for vegans, metformin users, long-term acid-reducer users, post-bariatric patients, and heavy alcohol intake, where B needs are higher.
This formula uses activated forms: methylcobalamin (B12 already in its bioactive form), L‑5‑MTHF (folate your cells can use directly), P5P (vitamin B6 as pyridoxal‑5′‑phosphate), and riboflavin‑5′‑phosphate. These skip common activation bottlenecks and feed the enzymes that turn carbs, fat, and protein into usable energy. The generous niacin dose reduces how much fat your liver releases as energy-poor byproducts and improves cellular energy reactions, while B6, folate, B12, and choline help recycle Homocysteine toward methylation (the cell’s on/off switches for many processes).
Take one capsule with breakfast; add a second with lunch if your clinician advises more. Morning matters because B vitamins can feel stimulating. Food reduces nausea and softens niacin flush. If you flush, it’s harmless warmth and tingling that fades in 20–40 minutes; splitting doses or taking with a full meal helps. Recheck Vitamin B12, MMA, Homocysteine, and RBC Folate after 4 to 8 weeks to confirm you’re in range, then consider stepping down to the lowest dose that maintains your labs.
Immediate-release niacin at this level can worsen gout by raising uric acid and can nudge glucose higher in diabetes; monitor if these apply. Skip if you’ve had a niacin hypersensitivity reaction. Levodopa alone (without carbidopa) can be weakened by vitamin B6; if you use carbidopa/levodopa, this is less of an issue. Folate can mask anemia from low B12, which is why pairing L‑5‑MTHF with methylcobalamin is appropriate here. Pregnancy requires dedicated prenatal dosing; this isn’t a prenatal.
How fast will you feel it? Energy and concentration often improve within 1 to 2 weeks if low B status was part of the problem, while lab markers shift over 4 to 8 weeks. Is “methylated” better? If you have trouble activating folate or B12, L‑5‑MTHF and methylcobalamin are the forms most clinicians choose. Can a B complex cause insomnia? Sometimes—take it earlier in the day.
Frequently asked questions
What does a B complex do for energy?
B vitamins act as coenzymes that help your cells convert carbs, fat, and protein into usable energy. If your B12, MMA, Homocysteine, or RBC Folate suggest low status, correcting it can translate to steadier energy within 1–2 weeks.
Should I take B complex in the morning or at night?
Morning is best. B vitamins can feel stimulating in some people, so taking them with breakfast, and again at lunch if needed, reduces the chance of sleep disruption.
Will this B complex cause niacin flush?
It can. The 140 mg niacin is immediate‑release and may cause a warm, red, tingling flush for 20–40 minutes. Taking with food, splitting the dose, or using aspirin only if approved by your clinician can lessen it.
Is a methylated B complex better if I have an MTHFR variant?
Yes. L‑5‑MTHF and methylcobalamin bypass common activation steps, which is helpful if your folate activation is less efficient. Many clinicians prefer these forms when Homocysteine runs high.
How long until B12 and folate labs improve?
Vitamin B12, MMA, Homocysteine, and RBC Folate typically move in the right direction within 4–8 weeks. Retest then, and adjust to the lowest dose that maintains good labs and symptoms.
Can I take B complex with metformin or acid reducers?
Yes, and it’s often sensible. Metformin and long‑term acid reducers can lower B12 absorption. This formula includes methylcobalamin, but still verify with Vitamin B12 and MMA testing.
Is this B complex safe in pregnancy?
It provides L‑5‑MTHF, but it isn’t a complete prenatal. Pregnancy typically needs dedicated prenatal dosing and added nutrients like iron and iodine. Use a prenatal and follow your obstetrician’s guidance.
Can B complex interact with my medications?
Vitamin B6 can reduce the effect of levodopa when taken without carbidopa. Niacin can worsen gout and can affect glucose. If you take these meds or have these conditions, discuss dosing and monitoring with your clinician.
How to take it & ingredients
Suggested use: Take 1 capsule one to three times daily or as recommended by your health professional.
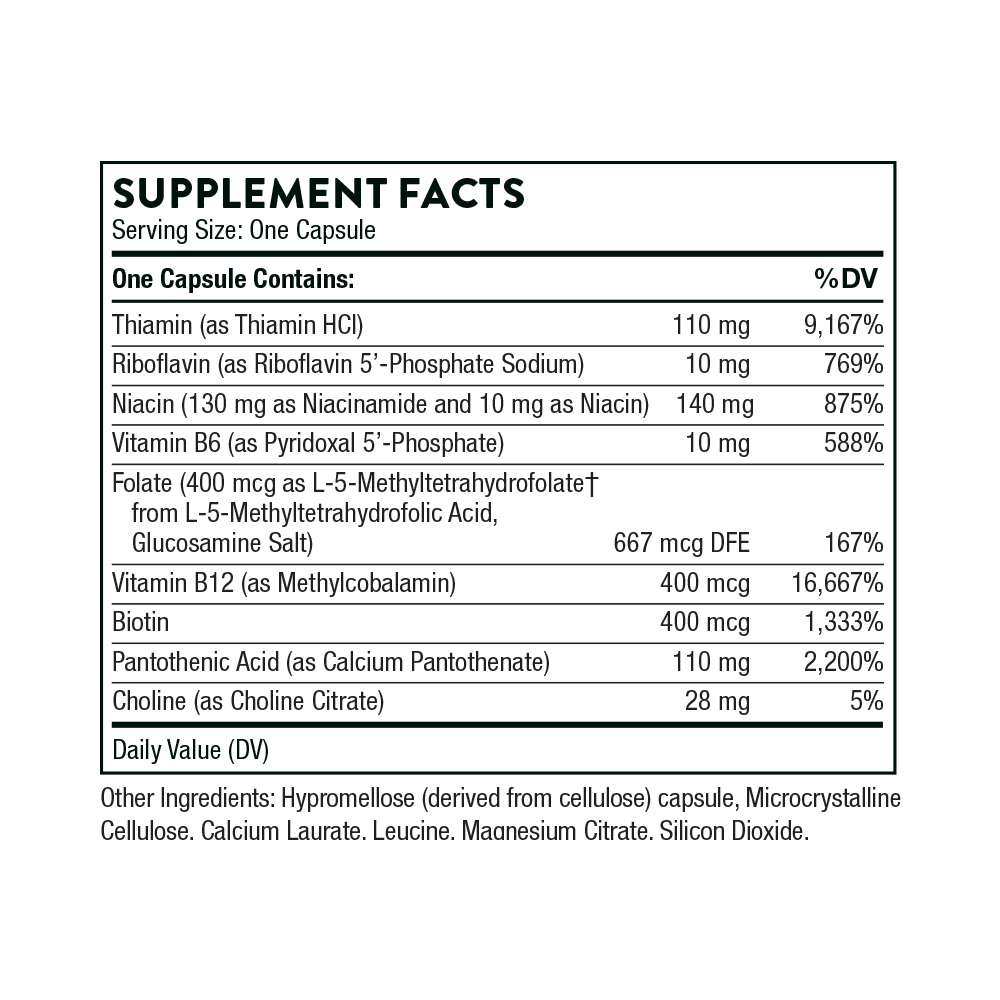
Active ingredients
1 capsule per serving · 60 servings
Thiamin
Thiamin HCI
Thiamin HCI
110 mg
Riboflavin
Riboflavin 5'-Phosphate Sodium
Riboflavin 5'-Phosphate Sodium
10 mg
Choline
Choline Citrate
Choline Citrate
28 mg
Folate
L-5-Methyltetrahydrofolate from L-5-Methyltetrahydrofolic, Glucosamine Salt
L-5-Methyltetrahydrofolate from L-5-Methyltetrahydrofolic, Glucosamine Salt
400 mcg
Vitamin B12
Methylcobalamin
Methylcobalamin
400 mcg
Biotin
400 mcg
▼
Niacin
140 mg
Niacin
Niacinamide
Niacinamide
130 mg
Niacin
Niacin
Niacin
10 mg
Vitamin B5
Calcium Pantothenate
Calcium Pantothenate
110 mg
Vitamin B6
Pyridoxal 5'-Phosphate
Pyridoxal 5'-Phosphate
10 mg
Other ingredients: Calcium Laurate, Hypromellose Capsule, Leucine, Magnesium (Citrate), Microcrystalline Cellulose, Silicon Dioxide
Certifications
Benefits
Warnings