


Allergy Research Group
Laktoferrin 350mg by Allergy Research Group
120 capsules · 120-day supply
Natural Immune Support with Lactoferrin for Overall Wellness$159.99
Purchase options
Practitioner-grade brand3rd-party testedFree shipping $50+
Allergy Research Group Laktoferrin 350mg overview
If your Ferritin (the iron storage marker) stays low despite taking oral iron, lactoferrin is a smart add-on. It’s helpful for menstruating adults with low Hemoglobin, athletes with heavy training loads, and postpartum women rebuilding iron. It also fits people with sensitive digestion who don’t tolerate high-dose iron. If your Ferritin is already high or you have hemochromatosis, skip lactoferrin for iron and talk with your clinician.
Lactoferrin is an iron-binding protein from milk. In the gut it escorts iron to where it’s absorbed, while tying up excess “free” iron that feeds harmful microbes. Human studies suggest it can lower hepcidin (the liver hormone that blocks iron absorption), which is one reason Ferritin and Hemoglobin can rise over 4 to 12 weeks. By limiting iron to pathogens, lactoferrin also helps with microbiome balance and modestly lowers hs-CRP (an inflammation marker) in some responders.
The suggested use is 1 to 3 capsules at night before bed. That timing keeps it away from large calcium-rich meals that compete with iron handling. If you’re repleting iron, pairing lactoferrin with a lower-dose iron supplement earlier in the day often improves tolerance versus pushing iron alone. Recheck Ferritin and Hemoglobin after 8 to 12 weeks, then taper to a maintenance dose once your levels are solid.
Avoid lactoferrin if you have a true cow’s milk protein allergy. It’s typically very low in lactose, but strict dairy-free vegans may still prefer to avoid it. If your Ferritin or Transferrin Saturation (how full your iron carriers are) is high, or you have hemochromatosis or are on iron chelation, do not use it for iron. Pregnancy and nursing: commonly used, but confirm dosing with your OB before starting.
Frequently asked questions
What is lactoferrin good for?
Lactoferrin helps iron absorption and transport while limiting iron to harmful microbes in the gut. In iron-deficient adults, it can raise Ferritin and Hemoglobin over 4–12 weeks and may modestly lower hs-CRP. It’s also used to support microbiome balance.
Can I take lactoferrin with iron supplements?
Yes. They’re often combined. Many clinicians use lactoferrin alongside a moderate iron dose to improve absorption and tolerance. Separate from large calcium doses. Recheck Ferritin and Hemoglobin after 8–12 weeks to adjust.
How long does lactoferrin take to raise ferritin?
Expect changes within 4 to 12 weeks if you’re truly low on iron and your intake is adequate. Rate of rise depends on baseline Ferritin, ongoing blood loss (heavy periods), and whether inflammation is elevating hepcidin.
Does lactoferrin help with H. pylori or gut infections?
It can help as an adjunct by restricting iron that microbes need. Some studies show better eradication rates for H. pylori when added to standard therapy. It’s not a stand-alone treatment; follow your clinician’s plan.
Is lactoferrin safe in pregnancy and breastfeeding?
Generally considered safe and widely used for iron support in pregnancy, but dosing should be set by your OB. If you have high Ferritin or a history of iron overload, do not start without medical guidance.
Is lactoferrin dairy-free and OK for lactose intolerance?
It’s derived from milk proteins, so avoid if you have a milk protein allergy. Lactose content is typically minimal, and most people with lactose intolerance tolerate it, but stop if you notice GI symptoms.
What side effects can lactoferrin cause?
It’s usually well tolerated. Occasional nausea, mild GI upset, or constipation can occur, especially when paired with iron. Taking it away from large meals and adjusting iron dose usually helps.
Does lactoferrin interact with medications?
No major drug interactions are known. If you’re on iron chelation therapy or have iron overload, avoid lactoferrin. As with any supplement, review with your clinician if you take multiple medications.
How to take it & ingredients
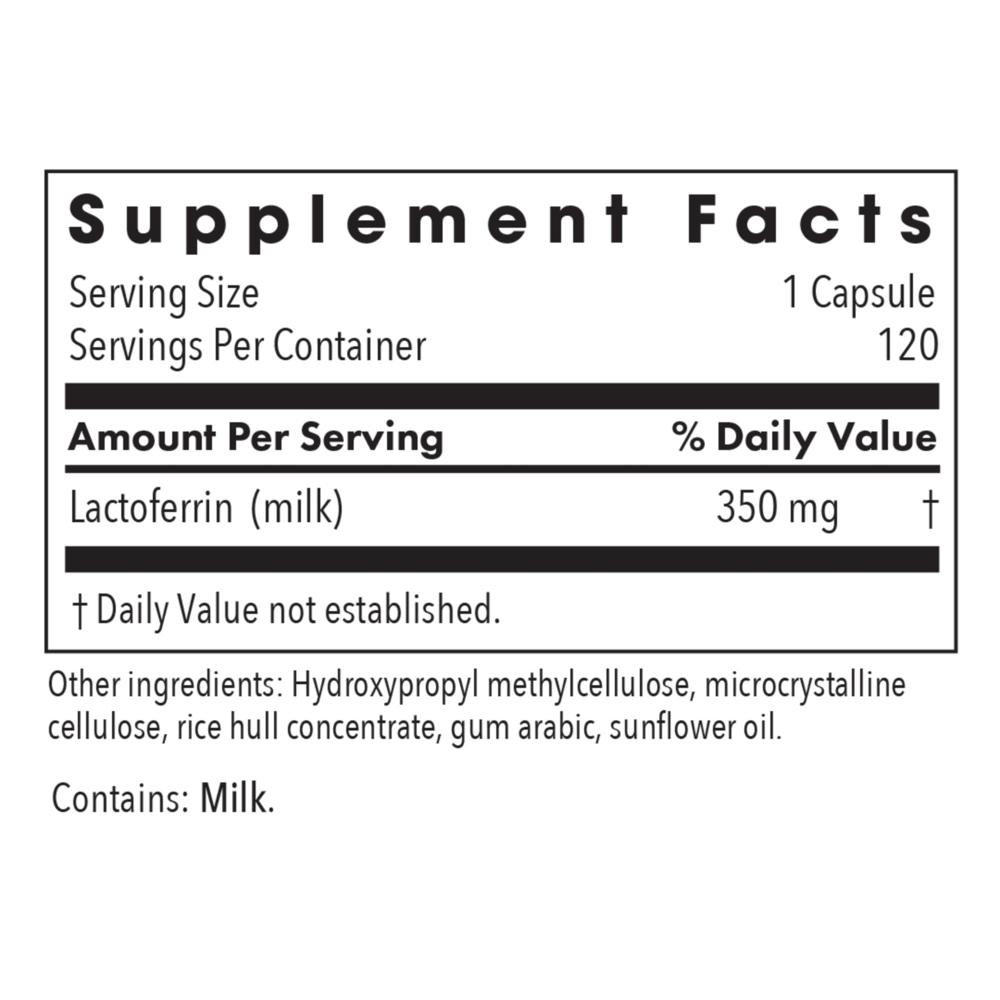
Suggested use: As a dietary supplement, 1 to 3 capsules at night before bed, or as directed by a healthcare practitioner.
Active ingredients
1 capsule per serving · 120 servings
Lactoferrin
From milk
From milk
350 mg
Other ingredients: Hydroxypropyl methylcellulose, Microcrystalline cellulose, Rice hull concentrate, Gum arabic, Sunflower oil
Certifications
Benefits
Warnings
Customers also considered

NK-Stim
Ortho Molecular Products
60 capsules
$72.54Save 10% with Subscribe & Save

OrthoMune®
Ortho Molecular Products
120 capsules
$67.10Save 10% with Subscribe & Save

Phytocidal
Ortho Molecular Products
120 capsules
$100.07Save 10% with Subscribe & Save
PureDefense w/Nac
Pure Encapsulations
20 capsules
$19.00Save 21% with Subscribe & Save