

Amen
Zinc/Copper + Probiotics by Amen
90 capsules · 90-day supply
Essential Zinc and Copper with Probiotics for Immune and Digestive Support$24.99
Purchase options
Practitioner-grade brand3rd-party testedFree shipping $50+
Vegan·Vegetarian
Amen Zinc/Copper + Probiotics overview
This is a fit if you need a zinc and copper supplement that won’t unbalance the two. It suits adults with low zinc on labs (Zinc, Plasma or Serum), diets high in whole grains/legumes that bind zinc, post-bariatric patients, or heavy exercisers with high sweat loss. If your Copper, Serum or ceruloplasmin (the main copper-carrying protein) runs low-normal, the built-in copper helps protect against zinc-driven depletion. For long-term maintenance, most people later step down to a lower zinc dose.
Zinc picolinate is a chelated form paired with picolinic acid that’s well absorbed compared with oxide or gluconate. Zinc and copper compete for the same intestinal transporters, and high zinc induces metallothionein (a metal-binding protein) that traps copper, so adding 2 mg of copper glycinate preserves balance. Bacillus subtilis is a spore-forming probiotic that survives stomach acid, can produce digestive enzymes, and modestly shifts gut communities; some users see steadier digestion and less gas.
Take one capsule daily with water; food reduces the chance of zinc-related nausea. Fifty milligrams is a repletion-level dose, typically used for 4 to 12 weeks while you recheck Zinc, Plasma or Serum and Copper, Serum or ceruloplasmin. For ongoing upkeep after levels normalize, a lower zinc dose (often 10–15 mg with ~1 mg copper) is usually more appropriate. Separate from iron, calcium, coffee, and high-phytate meals by a couple of hours to improve absorption.
Zinc binds certain medications: separate by at least 2–6 hours from tetracycline and quinolone antibiotics, levothyroxine, and penicillamine. If you also take iron, alternate times of day. Chronic high-dose zinc without monitoring can lower copper and cause anemia on a Complete Blood Count; the added copper reduces this risk but labs still matter. Skip copper-containing products if you have Wilson’s disease or unexplained high copper, and discuss with your clinician if you have significant liver disease.
Frequently asked questions
Is 50 mg of zinc too much to take every day?
It’s a high, repletion-level dose. Many clinicians use 25–50 mg daily for several weeks in those with low zinc, then step down. Long-term daily use at 50 mg without monitoring can deplete copper and affect blood counts; recheck labs and taper when levels normalize.
Do I need copper when I take zinc?
Yes at higher zinc doses. Zinc and copper compete for absorption, and high zinc can drive copper down. Including about 1–2 mg of copper with repletion-level zinc helps maintain balance; confirm with Copper, Serum or ceruloplasmin testing.
Can I take zinc with antibiotics or thyroid medicine?
Not together. Zinc reduces absorption of tetracycline and quinolone antibiotics and levothyroxine. Separate by at least 2–6 hours. If you’re unsure which class your antibiotic is, ask your pharmacist before combining.
Does zinc cause nausea or stomach upset?
It can, especially on an empty stomach. Take with food and a full glass of water. If nausea persists, try a smaller meal, switch timing, or discuss lowering the dose once your labs improve.
Does Bacillus subtilis need refrigeration?
No. It’s a spore-forming probiotic that’s heat-stable and survives stomach acid. Store at room temperature away from moisture. Consistent daily use is more important than exact timing with meals.
How long until I notice effects from zinc?
Lab changes often show within 4–8 weeks. Immune and skin benefits, if due to low zinc, may track with that timeline. If taste or smell changes are from deficiency, improvement can appear sooner, but causes vary, so don’t rely on zinc alone without evaluation.
Can I take this with iron or calcium?
Yes, just not at the same time. Minerals compete for absorption. Take zinc at a different time of day from iron or calcium, ideally separated by 2 hours or more.
Is this zinc and copper combo safe in pregnancy?
Fifty milligrams of zinc is above typical prenatal doses. Use only if there’s a documented need and clinician guidance, then step down once levels normalize. Prenatal vitamins already contain copper, so avoid doubling up without checking total intake.
How to take it & ingredients
Suggested use: Take one capsule daily with 8 ounces of water or your preferred beverage. May be taken with or without food.
Active ingredients
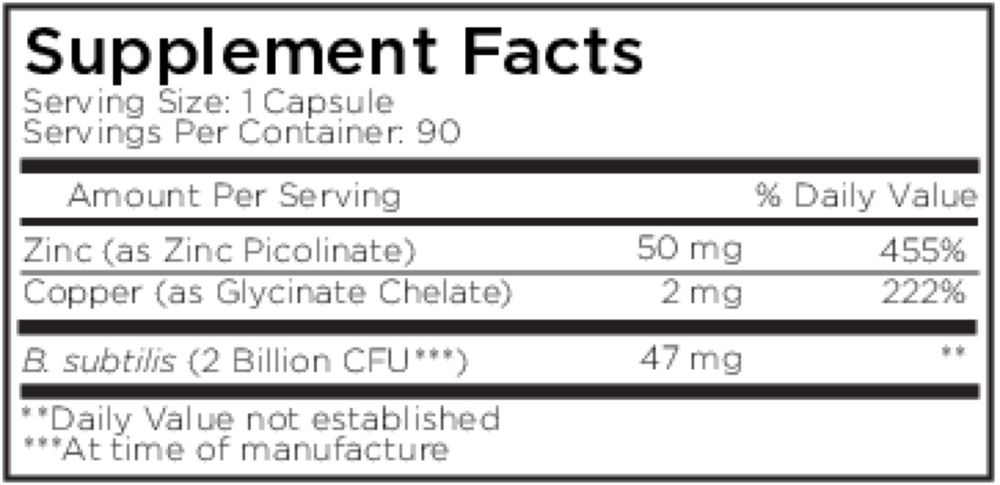
1 capsule per serving · 90 servings
Zinc
Zinc Picolinate
Zinc Picolinate
50 mg
Copper
Copper Glycinate Chelate
Copper Glycinate Chelate
2000 mcg
Bacillus subtilis
2 billion CFU, 47 mg
Other ingredients: Methylcellulose capsule
Certifications
Benefits
Warnings