



Argentyn 23
Silver Hydrosol Argentyn 23 Pro 115 mcg by Argentyn 23
236 milliliters · 47-day supply
Bio-Active Silver Hydrosol, 23 ppm$55.99
Purchase options
Practitioner-grade brand3rd-party testedFree shipping $50+
Gluten Free
Argentyn 23 Silver Hydrosol Argentyn 23 Pro overview
This silver hydrosol suits adults who already use a daily wellness routine and want a sublingual liquid format to round it out. The formula is intentionally minimal, just two ingredients: bio-active silver and pharmaceutical-grade purified water meeting USP-NF standards. It is a low-concentration hydrosol rather than a megadose product.
Each adult serving of one teaspoon (5 mL) delivers 115 mcg of silver at a concentration of 23 ppm. The hydrosol uses an ultra-fine dispersion with particle sizes as small as 0.8 nanometers, validated by transmission electron microscopy, and greater than 98 percent of the silver is present as positively charged bio-active ions and nanoclusters. The low concentration paired with the small particle size is the manufacturer's stated approach to absorption and elimination.
Suggested use is one teaspoon for adults, held under the tongue for about 30 seconds, then swallowed. Children four years and older take half a teaspoon. Take silver products separately in time from oral medications and minerals (a two to four hour gap is a common spacing), since metals can bind compounds in the gut. Use the dropper or cap to measure rather than estimating from the bottle.
If you are pregnant or breastfeeding, take prescription medications, or have a clinician managing your care, talk to your care team before starting and review the warnings below.
Frequently asked questions
What is bio-active silver hydrosol?
A liquid silver product where the silver is dispersed in pharmaceutical-grade purified water as ultra-fine particles, with greater than 98 percent present as positively charged ions and nanoclusters. The manufacturer uses this format to keep particle size small while concentration stays low at 23 ppm.
How much silver is in one teaspoon?
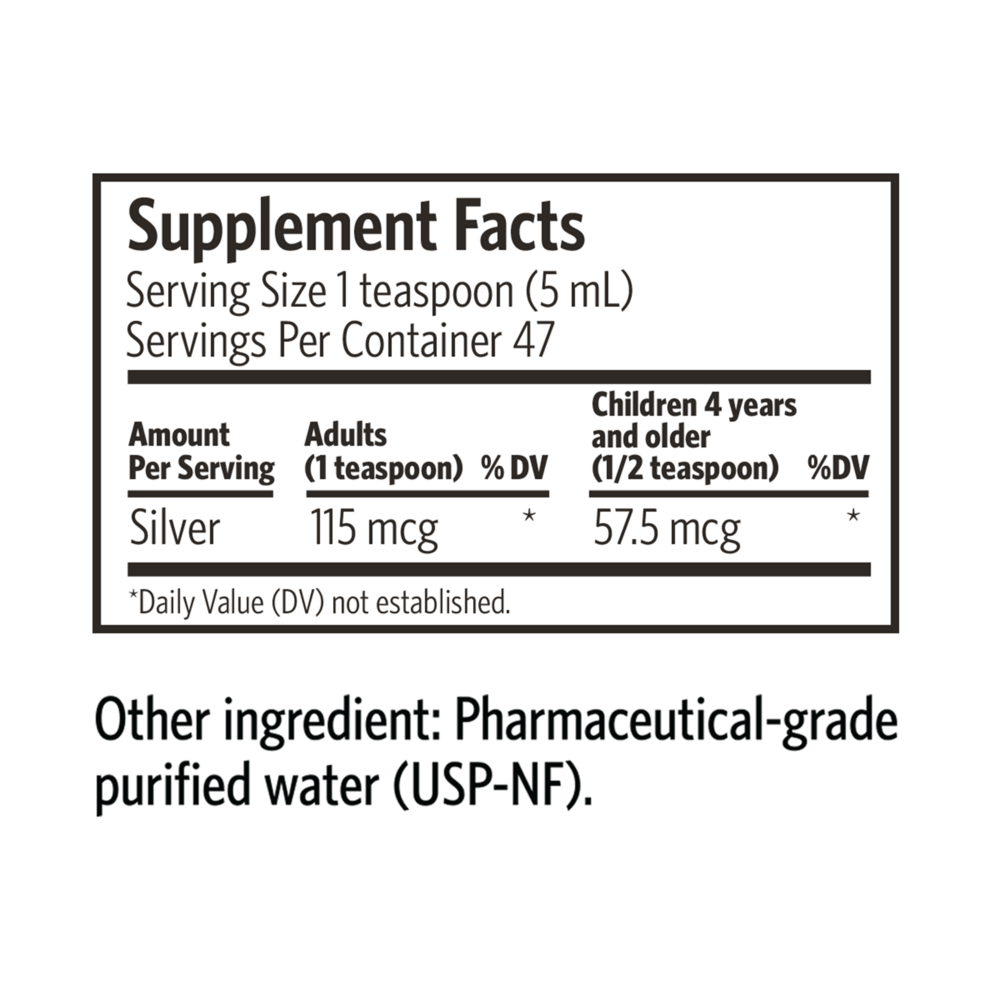
Each adult teaspoon (5 mL) delivers 115 mcg of silver. Children four years and older take half a teaspoon, which delivers 57.5 mcg. The Daily Value for silver has not been established because silver is not a nutrient.
How do I take this hydrosol?
The manufacturer's suggested use is one teaspoon held under the tongue for about 30 seconds, then swallowed. Use the dropper or cap to measure. Take it separately in time from prescription medications and mineral supplements.
How is this different from other silver products?
The manufacturer's stated points of difference are the ultra-fine particle dispersion (as small as 0.8 nm, validated by transmission electron microscopy), the greater than 98 percent bio-active ion fraction, the two-ingredient formula, and the low 23 ppm concentration.
Should I separate this from other supplements?
Silver may bind minerals and some oral medications in the gut. A common spacing is two to four hours from thyroid hormone, oral antibiotics, iron, calcium, and zinc supplements.
Can I use it every day?
The manufacturer's suggested use allows for daily use. If you take it daily over many months, discuss long-term use with your clinician, since cumulative silver intake over long periods is associated with argyria (see warnings).
Is this product certified?
The water used in the formula meets USP-NF pharmaceutical-grade purified water standards. The manufacturer also notes that particle size is validated by transmission electron microscopy.
How to take it & ingredients
Suggested use: Adults: 1 teaspoon, hold under tongue for 30 seconds, then swallow. Children 4 years and older: 1/2 teaspoon.
Active ingredients
1 teaspoon = 5 milliliter per serving · 47 servings
Silver
115 mcg
Other ingredients: Pharmaceutical-grade purified water
Certifications
Benefits
Warnings
Customers also considered

Laktoferrin 350mg
Allergy Research Group
90 capsules
$131.99Save 20% with Subscribe & Save

NK-Stim
Ortho Molecular Products
60 capsules
$72.54Save 10% with Subscribe & Save

OrthoMune®
Ortho Molecular Products
120 capsules
$67.10Save 10% with Subscribe & Save

Phytocidal
Ortho Molecular Products
120 capsules
$100.07Save 10% with Subscribe & Save