



Biocidin Botanicals
G.I. Detox 500 mg by Biocidin Botanicals
60 capsules · 60-day supply
Natural Detox Support for a Healthy Gut Environment$34.99
Purchase options
Practitioner-grade brand3rd-party testedFree shipping $50+
Vegan·Vegetarian·Gluten Free·Soy Free·Dairy Free·Milk Free·
Biocidin Botanicals G.I. Detox overview
This fits people running a gut protocol who feel worse when antimicrobials kick up die‑off, or anyone with stubborn bloating and loose stools after travel or food poisoning. A gut detox binder is also used under clinician guidance during mold or water‑damaged building exposure. If your Omega-3 Index and Vitamin D, 25-Hydroxy are fine but you still feel “inflamed,” a short binder trial can be reasonable while you track hs-CRP (a general inflammation marker) for trend, not as a cure-all.
Binders stay in the gut and latch onto charged particles and large molecules, then leave in the stool. That includes bile acids (detergent-like fats that can irritate the colon), bacterial fragments like LPS (lipopolysaccharide, a cell-wall piece that can trigger immune signaling), and some gas-producing byproducts. By reducing recirculation through enterohepatic circulation (the loop where bile and other compounds are reabsorbed), they can ease bloating and urgency without being absorbed into the bloodstream.
Take 1 capsule on an empty stomach with a full glass of water, at least 1 hour away from all medications and supplements; many clinicians prefer 2 hours for critical drugs. Start once daily for a few days, then consider twice daily if needed. Most people notice changes in bloating or stool consistency within 1 to 3 days. Hydration and adequate magnesium and fiber help prevent constipation during use.
Binders can reduce absorption of medications and nutrients. Space carefully from thyroid hormone, antibiotics, antifungals, seizure medications, HIV therapy, transplant immunosuppressants, and oral contraceptives. Separate from iron, zinc, calcium, and fat-soluble vitamins (A, D, E, K) as well as probiotics. If you take evening meds, use the binder earlier in the day, and keep the window consistent.
Avoid during pregnancy or breastfeeding unless your clinician directs it. Skip if you have chronic constipation, bowel obstruction history, severe motility disorders, recent GI surgery, or active GI bleeding. If you’re iron deficient or have low Ferritin (your iron storage marker), long-term daily binder use isn’t appropriate without monitoring. For ongoing diarrhea with fever, blood, or weight loss, get evaluated first.
Frequently asked questions
How long does a gut binder take to work?
For bloating or loose stools, many notice a change within 1–3 days. For use during antimicrobial or mold protocols, it’s often taken throughout the protocol and tapered once symptoms and exposures settle.
Can I take a binder with antibiotics or thyroid meds?
Yes, but never at the same time. Separate by at least 2 hours to avoid reduced absorption. If a medication is mission‑critical, ask your prescriber for a personalized spacing plan.
Does a GI detox binder cause constipation?
It can, especially if you’re under-hydrated. Drink a full glass of water with each dose, keep daily fluids up, and ensure adequate magnesium and fiber. If constipation persists, reduce the dose or stop.
Will a binder deplete vitamins and minerals?
It can lower absorption if taken together. Take your multivitamin, iron, zinc, and fat‑soluble vitamins at a different time window. Long-term daily use should be supervised and labs like Ferritin monitored.
Is a gut detox binder safe to use every day?
Short courses are typical. Daily long-term use should be guided by a clinician with a plan and periodic review. Address root causes like diet, infections, or exposures rather than relying on a permanent binder.
Can I open the capsule and mix it with water?
Usually yes, the contents can be mixed with water if swallowing capsules is difficult. The taste and texture can be gritty. Still take it away from medications and supplements.
Will a binder help with diarrhea after gallbladder removal?
Sometimes. Binders can sequester irritating bile acids in the colon. If diarrhea is persistent after cholecystectomy, discuss options with your clinician; prescription bile acid binders may be more effective.
How to take it & ingredients
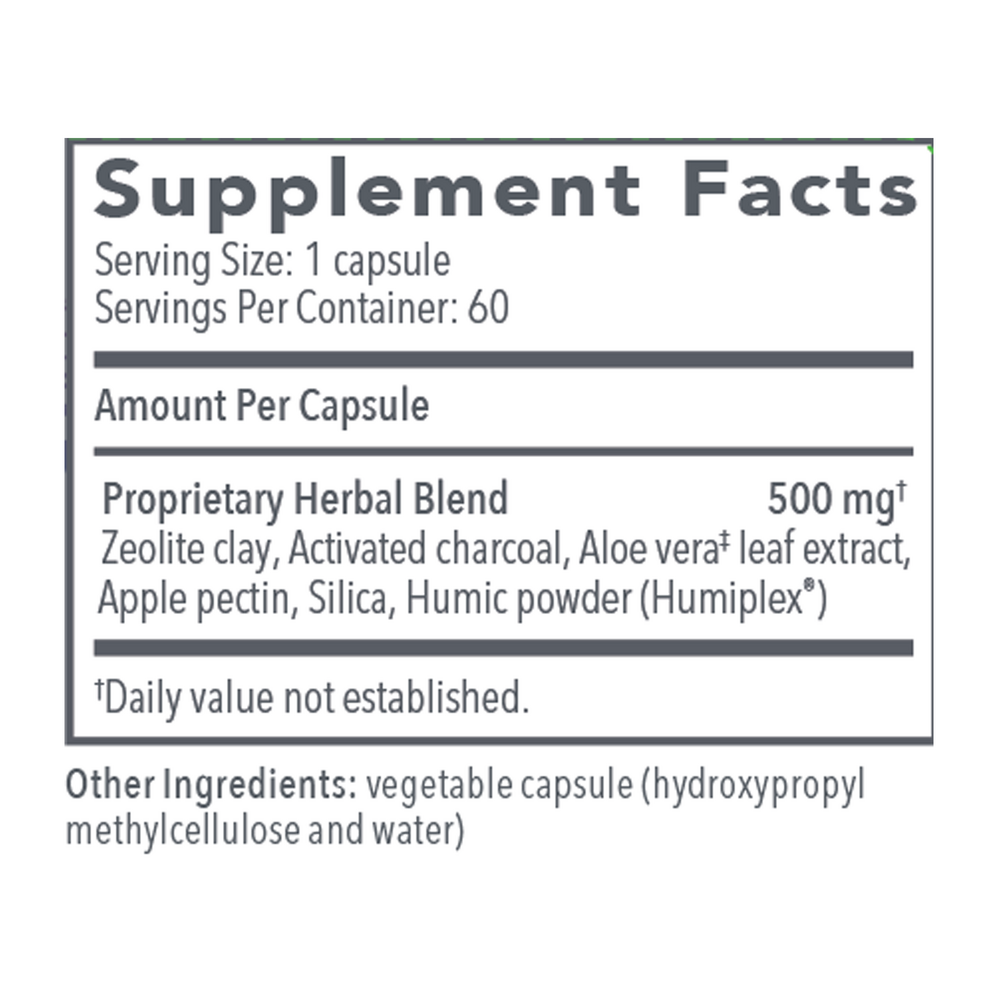
Suggested use: Take 1 capsule on an empty stomach with a full glass of water or as directed by a healthcare professional. Take at least 1 hour apart from medications and supplements.
Active ingredients
1 capsule per serving · 60 servings
▼
Proprietary Herbal Blend
500 mg
Zeolite Clay
-
Activated Charcoal
-
Aloe Vera Leaf Extract
-
Apple Pectin
-
Silica
-
Humic Powder
-
Other ingredients: Vegetable capsule (hydroxypropyl methylcellulose, water)
Certifications
Benefits
Warnings
