


Eye Promise
EyePromise EZ Tears by Eye Promise
60 softgels · 30-day supply
Comprehensive Support for Dry Eyes and Overall Eye Health$42.99
Purchase options
Practitioner-grade brand3rd-party testedFree shipping $50+
Gluten Free·Yeast Free
Eye Promise EyePromise EZ Tears overview
If screens, contact lenses, or post-LASIK dryness leave your eyes gritty by afternoon, an omega-3–based dry eye supplement fits. It’s most useful when seafood intake is low or your Omega-3 Index (a blood test of EPA/DHA in red cells) is low. People with meibomian gland issues (the oil glands that keep tears from evaporating) and peri- or postmenopausal adults tend to report the biggest gains within 4 to 12 weeks.
EPA and DHA (the long-chain omega-3 fats in fish oil) calm surface inflammation and improve the oily layer of the tear film, which slows evaporation. Vitamin A supports the corneal surface and goblet cells (the cells that make the mucin layer of tears). Vitamin D3 helps modulate immune activity at the ocular surface, and vitamin E protects these oils from oxidation. Clinically, some patients show lower hs-CRP (a blood inflammation marker) and less burning, though large trials in unselected dry eye have been mixed; in practice, response is better when omega-3 status is low or oil glands are plugged.
Take two softgels daily with a meal that contains fat for best omega-3 absorption. Consistency matters, as membranes in tear glands turn over slowly; give it 4 to 12 weeks. If you get fishy burps, take at night or briefly freeze the softgels. If your Omega-3 Index stays low or you also want triglyceride lowering, a higher EPA/DHA dose from a dedicated fish oil is often required. Keep warm compresses and eyelid hygiene in the mix.
This formula includes preformed vitamin A (retinyl palmitate). Avoid in pregnancy or if you could become pregnant unless your clinician approves, and be cautious with liver disease or if you already take retinoid drugs like isotretinoin or acitretin. Fish or shellfish allergy is a stop sign. If you use anticoagulants such as warfarin or high-dose aspirin, fish oil and vitamin E can increase bleeding risk, so check with your prescriber and monitor INR if applicable.
Frequently asked questions
Do omega-3 supplements actually help dry eye?
They help some people, especially with meibomian gland dysfunction and low seafood intake, but results are mixed in large trials. Clinically, many see less burning and better comfort after 4 to 12 weeks of steady EPA/DHA intake.
How long does it take for dry eye supplements to work?
Expect 4 to 12 weeks. Omega-3s need time to incorporate into the glands that produce the oily tear layer. If there’s no change by 12 weeks, reassess dose, Omega-3 Index, and eyelid care with your eye doctor.
Can I take this with blood thinners like warfarin?
Use caution. Fish oil and vitamin E can increase bleeding tendency. If you’re on warfarin or similar drugs, talk with your prescriber first and arrange extra INR checks when starting or changing the dose.
Is the vitamin A in this safe during pregnancy?
No. Preformed vitamin A (retinol/retinyl palmitate) is not recommended in pregnancy due to birth defect risk at higher intakes. Choose a prenatal without preformed vitamin A unless your clinician specifically advises it.
Will this lower my triglycerides too?
Not reliably at this dose. Triglyceride reduction typically needs 2–4 grams per day of EPA+DHA. This blend targets ocular comfort; use a clinically dosed fish oil if triglycerides are your goal and monitor your lipid panel.
What if I get fishy burps or reflux from fish oil?
Take it with a full meal, try bedtime dosing, or keep softgels in the freezer to reduce aftertaste. Splitting the dose can also help. Persisting reflux suggests trying a different fish oil or algal omega-3.
Is there a vegan alternative to fish oil for dry eyes?
Yes. Algal oil provides DHA and often EPA without fish. If you choose algal omega-3, recheck your Omega-3 Index after 8 to 12 weeks to confirm you’ve reached an effective level.
Is mercury a concern with fish oil?
Highly refined fish oils are purified to remove mercury and other contaminants. Look for products that follow IFOS, GOED, or USP standards. This category is generally considered low risk for mercury.
How to take it & ingredients
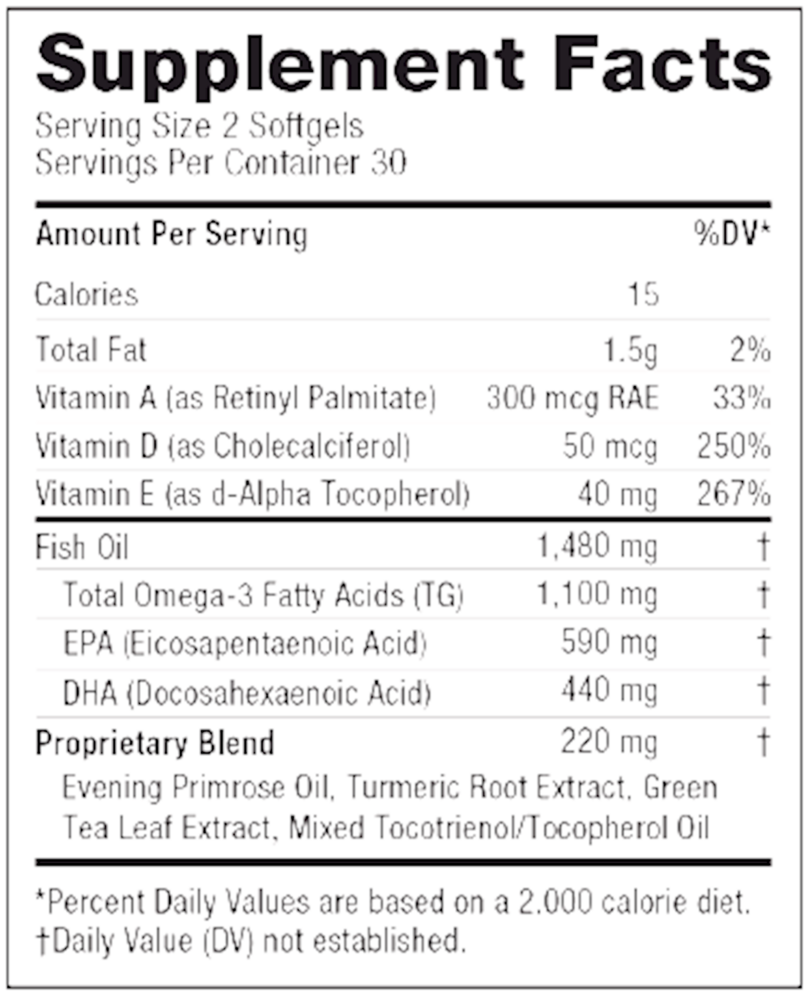
Suggested use: Adults take 2 softgels per day with a meal, or as directed by your eye care professional.
Active ingredients
2 softgels per serving · 30 servings
Vitamin A
As Retinyl Palmitate
As Retinyl Palmitate
300 mg
Vitamin D
As Cholecalciferol
As Cholecalciferol
50 mcg
Vitamin E
As d-Alpha Tocopherol
As d-Alpha Tocopherol
40 mg
▼
Fish Oil
1480 mg
▼
Total Omega-3 Fatty Acids
TG
TG
1100 mg
EPA
Eicosapentaenoic Acid
Eicosapentaenoic Acid
590 mg
DHA
Docosahexaenoic Acid
Docosahexaenoic Acid
440 mg
▼
Proprietary Blend
220 mg
Evening Primrose Seed Oil
-
Turmeric Root Extract
-
Green Tea Leaf Extract
-
Tocotrienol/Tocopherol Complex
-
Other ingredients: Gelatin, Glycerin, Yellow Beeswax, Purified Water, Annatto (color), Soy Lecithin Oil, Organic Extra Virgin Olive Oil, Corn Oil, Titanium Dioxide (color), Natural Orange Oil
Certifications
Benefits
Warnings
Customers also considered

4sight
Ortho Molecular Products
60 capsules
$106.95Save 10% with Subscribe & Save

EyePromise DVS
Eye Promise
60 softgels
$45.99Save 20% with Subscribe & Save

EyePromise Screen Shield Pro
Eye Promise
30 softgels
$39.99Save 20% with Subscribe & Save

EyePromise Zeaxanthin + Lutein
Eye Promise
60 softgels
$41.99Save 19% with Subscribe & Save