

Integrative Therapeutics
Active B-Complex by Integrative Therapeutics
120 capsules · 60-day supply
Comprehensive B Vitamin Support for Energy and Metabolism$35.99
Purchase options
Practitioner-grade brand3rd-party testedFree shipping $50+
Gluten Free·Soy Free·Dairy Free·Wheat Free·Artificial Color Free·Artificial Flavor Free
Integrative Therapeutics Active B-Complex overview
A methylated B complex fits people with low energy, elevated Homocysteine (an amino acid linked to vascular risk), or a history of low Vitamin B12 or Folate, especially if you carry common MTHFR gene variants that process folate less efficiently. It’s also useful if your Methylmalonic Acid (a marker of B12 status) is high, you’re on metformin or acid-suppressing meds that lower B12, or you follow a mostly plant-based diet. This dose is repletion-level for many adults; if your labs are severely low, work with a clinician, then step down to maintenance.
This formula uses 5-MTHF (methylfolate, the form your cells use directly) and methylcobalamin (an active B12), which feed methylation, the on–off tagging system your body uses to build neurotransmitters and recycle Homocysteine. Pyridoxal-5-phosphate (active B6) completes that cycle. Together they lower Homocysteine 20–30% in most responders within 4–8 weeks. Niacinamide (a non-flushing form of B3) supports energy metabolism without affecting lipids. Riboflavin and thiamin help convert carbs and fats to ATP, which is the energy currency in cells.
Take 1 capsule with breakfast; increase to 2 daily if guided by symptoms or labs. Food reduces nausea some people feel with B vitamins. Morning is best because B6 and B12 can feel stimulating. If you split the dose, take the second at lunch. Expect bright yellow urine from riboflavin. Recheck Vitamin B12, Folate, Homocysteine, and, if previously high, Methylmalonic Acid after 8–12 weeks to calibrate ongoing need.
If you take levodopa without carbidopa, high-dose B6 can reduce its effect. Folate can blunt methotrexate used for cancer; oncology patients should avoid extra folate unless directed. History of neuropathy warrants caution with B6, even at moderate doses. For pregnancy, use a prenatal; this B6 dose exceeds typical prenatal targets even though the 800 mcg DFE methylfolate is appropriate.
Frequently asked questions
Is a methylated B complex better if I have an MTHFR variant?
Usually yes. 5-MTHF bypasses the enzyme step affected by common MTHFR variants, making folate use more reliable. It’s most relevant if Homocysteine is high or prior folic acid didn’t move your labs.
How long does it take to lower homocysteine with B vitamins?
Most responders see meaningful drops within 4–8 weeks. Recheck Homocysteine around 8–12 weeks and adjust dose or add riboflavin if needed, since riboflavin can further help in certain MTHFR profiles.
Can I take a B complex at night?
You can, but morning is better. B6 and B12 can feel stimulating and sometimes cause vivid dreams. If sleep is affected, move the dose to breakfast or lunch.
Does this B complex cause flushing like niacin?
No. It uses niacinamide, a non-flushing form of B3. You still get support for cellular energy reactions, but without the skin flush typical of high-dose nicotinic acid.
Why is my urine bright yellow after taking B vitamins?
That’s riboflavin (vitamin B2). It’s harmless and reflects normal urinary excretion of excess B2. Color intensity doesn’t indicate effectiveness or deficiency.
Can I use this with metformin or acid-reducing meds?
Yes, and it’s often helpful. Metformin and long-term proton pump inhibitors are linked to lower B12. Monitor Vitamin B12 and Methylmalonic Acid and adjust the dose based on results.
Can B vitamins trigger acne or nausea?
Occasionally. High B12 and B6 can trigger breakouts in a small subset. Taking with food reduces nausea. If skin issues arise, reduce to 1 capsule or take every other day and reassess.
Is this safe during pregnancy or breastfeeding?
Use a prenatal instead. While methylfolate is appropriate, the B6 dose here is higher than typical prenatal targets. A prenatal balances B doses with iron, iodine, and choline needs.
How to take it & ingredients
Suggested use: Adults take 1 to 2 capsules daily or as recommended by a healthcare professional.
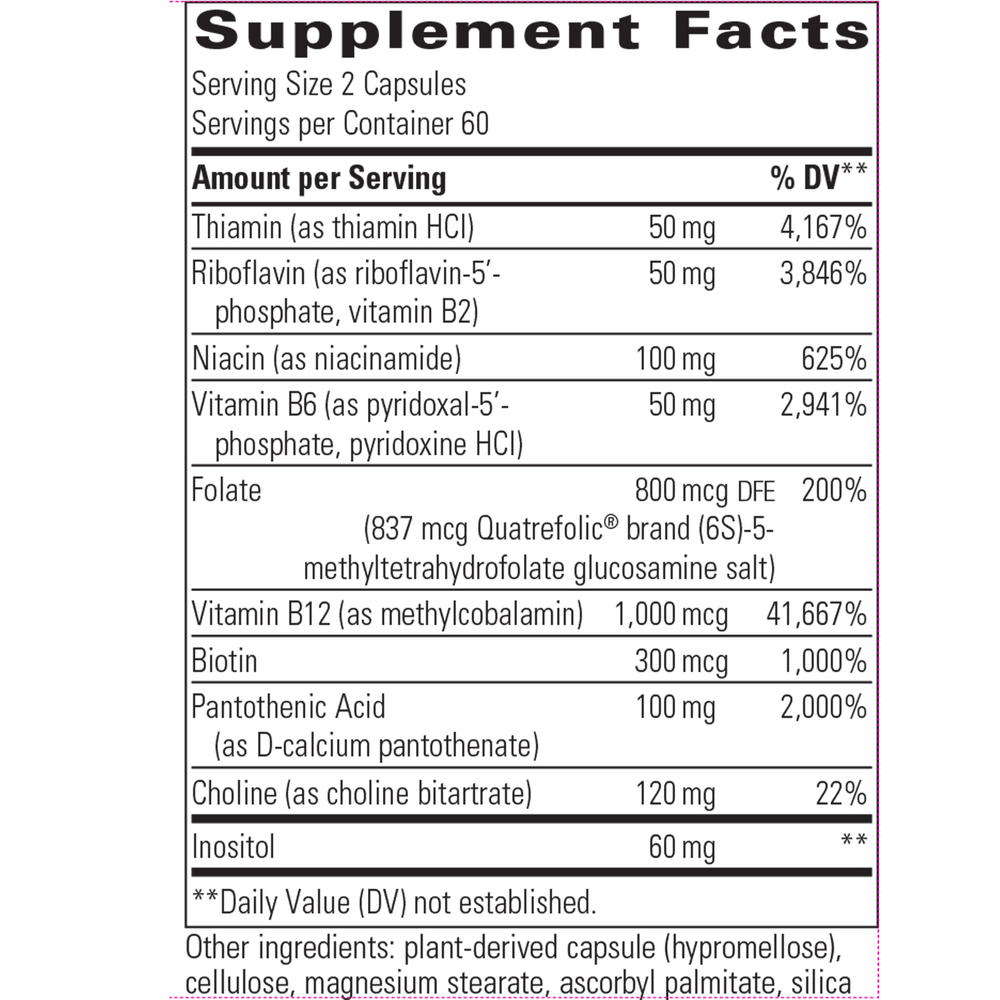
Active ingredients
2 capsules per serving · 60 servings
Thiamin
Thiamin HCl
Thiamin HCl
50 mg
Riboflavin
Riboflavin 5 phosphate and Vitamin B2
Riboflavin 5 phosphate and Vitamin B2
50 mg
Niacin
Niacinamide
Niacinamide
100 mg
Vitamin B6
Pyridoxal 5 phosphate and Pyridoxine HCl
Pyridoxal 5 phosphate and Pyridoxine HCl
50 mg
Folate
Quatrefolic (6S)-5 methyltetrahydrofolate glucosamine salt
Quatrefolic (6S)-5 methyltetrahydrofolate glucosamine salt
800 mcg DFE, 837 mcg
Vitamin B12
Methylcobalamin
Methylcobalamin
1000 mcg
Biotin
300 mcg
Pantothenic Acid
Calcium D pantothenate
Calcium D pantothenate
100 mg
Choline
Choline bitartrate
Choline bitartrate
120 mg
Inositol
60 mg
Other ingredients: Plant derived capsule (hypromellose), Cellulose, Magnesium stearate, Ascorbyl palmitate, Silica
Certifications
Benefits
Warnings



