


Klean Athlete
Calcium Citrate 300 mg by Klean Athlete
120 capsules · 60-day supply
Essential Calcium for Strong Bones and Optimal Muscle Function$XX.XX$22.50retail
Purchase option
20% below MSRP3rd-party testedFree shipping $50+
Vegan·Vegetarian·Gluten Free·Dairy Free·Egg Free·Fish Free·
Klean Athlete Calcium Citrate overview
If you’re choosing a calcium supplement because your diet is light on dairy or fortified foods, calcium citrate is the practical pick. It absorbs well even with low stomach acid, so it suits adults on proton pump inhibitors (acid-suppressing drugs for reflux), post‑menopausal women, vegans, and people after bariatric surgery. If your Vitamin D, 25-Hydroxy is low, fix that too—calcium works far better when vitamin D is replete. For those with a history of calcium oxalate stones, taking calcium with meals can reduce oxalate absorption.
Your skeleton is a mineral bank that your body deposits into and withdraws from, regulated by parathyroid hormone (the signal that pulls calcium from bone) and vitamin D. Calcium citrate provides elemental calcium to keep that balance steady, and the citrate part does not require much stomach acid to dissolve. In the gut it binds dietary oxalate, and in the urine citrate can reduce crystal formation, which is why clinicians often prefer citrate over carbonate in stone‑prone patients. Bone density shifts over months to years, not weeks.
Follow the label: 2 capsules with a meal, 1–3 times daily. Split doses of 300–500 mg at a time absorb better than one large dose. Take calcium citrate with food to pair it with dietary oxalate and improve uptake. Keep it a few hours apart from iron or zinc to avoid competition, and separate it from levothyroxine (thyroid medicine) and oral bisphosphonates by at least 4 hours. Check Vitamin D, 25-Hydroxy and aim for adequacy before judging calcium’s effect.
Calcium binds many drugs in the gut. Space it from levothyroxine, tetracycline or quinolone antibiotics, and oral bisphosphonates. Thiazide diuretics (blood‑pressure meds like hydrochlorothiazide) raise blood calcium; combining them with calcium supplements needs clinician oversight with periodic Calcium, Serum and possibly PTH checks. Large calcium doses can reduce absorption of iron and zinc—take those at a different time of day.
Avoid supplemental calcium if you have high blood calcium, untreated hyperparathyroidism, granulomatous diseases like sarcoidosis, or advanced kidney disease—get medical guidance first. If you form calcium phosphate stones, you still need meal‑time calcium, but total dose and 24‑hour urine calcium should guide use. If your dietary intake is already robust, extra calcium adds constipation and cost without bone benefit. Klean Athlete Calcium Citrate is best as a gap‑filler, not a blanket add‑on.
Frequently asked questions
Is calcium citrate better than calcium carbonate?
For many adults, yes—calcium citrate absorbs well without stomach acid, so it’s better if you’re on acid‑suppressing meds or older. Carbonate works if taken with meals and enough stomach acid is present. Both provide calcium; tolerance and context decide.
Should I take calcium citrate with or without food?
With food. Calcium taken with meals is absorbed more consistently and binds dietary oxalate, which can lower stone risk. It also helps limit nausea. Split your total into 300–500 mg doses rather than one large dose.
How much calcium citrate should I take per day?
Match the gap between your diet and your target intake. Many adults only need 300–600 mg from supplements if they eat some dairy or fortified foods. Higher repletion should be personalized with a clinician using diet review and, when relevant, DEXA scans.
Does calcium citrate cause constipation or gas?
Constipation can occur, though citrate is usually gentler than carbonate. Increase fluids and fiber, and consider magnesium at a separate time of day if you’re constipated. Gas or mild stomach upset typically improves when taken with meals.
Can I take calcium citrate with levothyroxine?
Yes, but separate them by at least 4 hours. Calcium binds levothyroxine in the gut and lowers its absorption, which can change your thyroid levels. Keep the timing consistent and recheck TSH after any schedule change.
Is calcium citrate safe if I’ve had kidney stones?
Often yes, and it’s typically preferred. Taken with meals, calcium citrate can lower oxalate absorption and urine stone risk. The details depend on your 24‑hour urine chemistry; share those results with your clinician to tailor dose and timing.
How long until calcium citrate helps my bones?
Bone density changes are slow. You’re building a foundation that’s measured over 1–2 years on DEXA, not weeks. Short‑term labs like Calcium, Serum and PTH reflect regulation, but diet, vitamin D status, and resistance exercise drive outcomes.
Can I take calcium citrate if I’m on a proton pump inhibitor (PPI)?
Yes. Calcium citrate does not rely on stomach acid for absorption, so it’s the usual choice for people on PPIs like omeprazole. Still take it with meals and consider checking Vitamin D, 25-Hydroxy to ensure you’re absorbing well.
How to take it & ingredients
Suggested use: As a dietary supplement, take 2 capsules, 1-3 times daily with a meal or as directed by a trainer, coach, or health professional.
Active ingredients
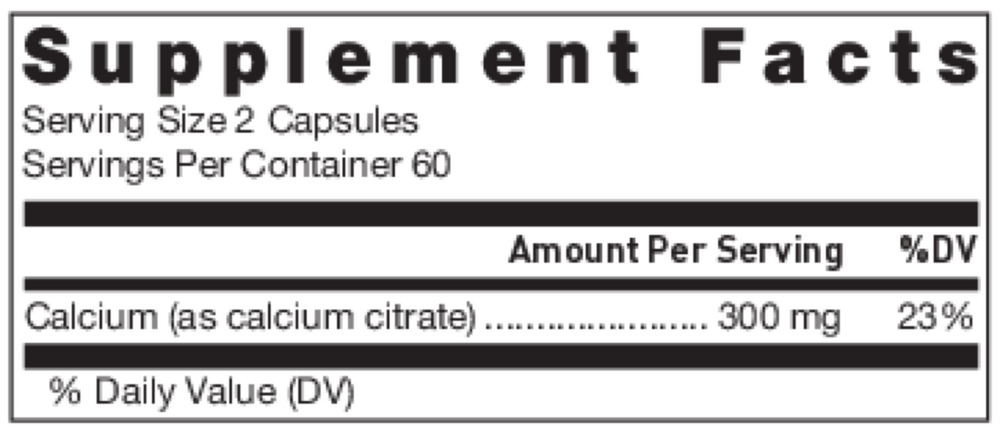
2 capsules per serving · 60 servings
Calcium
Calcium Citrate
Calcium Citrate
300 mg
Other ingredients: Capsule (hydroxypropyl methylcellulose, ascorbyl palmitate)
Certifications
Benefits
Warnings
Customers also considered

Thorne
Calcium
120 capsules
$XX.XX$28.00retail
Add to cart to see your price

Pure Encapsulations
Calcium Citrate
180 capsules
$XX.XX$32.50retail
Add to cart to see your price
Solaray
Calcium Citrate 1g
240 capsules
$XX.XX$26.99retail
Add to cart to see your price

Ortho Molecular Products
Reacted Calcium
180 capsules
$XX.XX$63.88retail
Add to cart to see your price