


Natura Health Products
VITAMIN D-A-K by Natura Health Products
60 capsules · 60-day supply
Essential Vitamins for Bone, Immune, and Cellular Support$24.99
Purchase options
Practitioner-grade brand3rd-party testedFree shipping $50+
Gluten Free·Soy Free·Egg Free·Milk Free·Tree Nut Free·Artificial Preservative Free·
Natura Health Products VITAMIN D-A-K overview
If your Vitamin D, 25-Hydroxy is in the lower part of the normal range and you get little midday sun, vitamin D3 K2 is a practical daily pick. It suits darker‑skinned adults, those at northern latitudes, dairy-free eaters, and post‑menopausal women prioritizing bone strength. The 125 mcg D3 here is a higher maintenance dose; for established deficiency, many people need a short clinician‑guided loading phase, then step down. Including vitamin A as beta‑carotene helps cover intake if you eat little liver, eggs, or orange vegetables.
D3 increases calcium absorption from the gut and brings down parathyroid hormone (the signal that pulls calcium from bone). Vitamin K1 and K2 switch on osteocalcin (the protein that locks calcium into bone) and matrix Gla protein (a protein that helps keep calcium out of arteries). This formula uses K2 as menaquinone-4 (MK-4), the fast-acting form used in many bone studies. Vitamin A here is beta-carotene, a precursor your body converts as needed, avoiding the bone-harming effects seen with excess preformed retinol.
Take 1 capsule daily with a meal that contains fat for better absorption. Morning or evening is fine. Most people see Vitamin D, 25-Hydroxy move within 4 to 12 weeks, so plan to recheck at 8–12 weeks and adjust with your clinician. If your level is already high-normal, this daily amount can overshoot over time; consider spacing doses or using a lower-strength D3 under guidance.
Skip or coordinate closely if you take warfarin or other vitamin K–antagonist blood thinners, since K1/K2 can lower the drug effect and change INR (the lab that tracks clotting time). Fat-blocking or bile-binding drugs like orlistat or cholestyramine reduce absorption; separate by 3–4 hours and monitor levels. Thiazide diuretics plus high vitamin D can raise blood calcium, so check calcium if you use this combo.
Use only with clinician oversight if you have a history of high calcium, recurrent calcium kidney stones, primary hyperparathyroidism, or granulomatous diseases like sarcoidosis, where extra D3 can raise calcium unpredictably. If you are pregnant or breastfeeding, the beta-carotene form of vitamin A is generally appropriate, but confirm dosing with your obstetric clinician.
Frequently asked questions
What does vitamin D3 K2 actually do?
D3 helps you absorb calcium and lowers parathyroid hormone, while K1/K2 activate proteins that put calcium into bone and keep it out of arteries. Together they improve calcium handling, which is why they’re paired for bone health.
How long does it take to raise my Vitamin D, 25-Hydroxy?
Expect movement within 4–12 weeks. Recheck your Vitamin D, 25-Hydroxy at 8–12 weeks and adjust. If your level is very low or body weight is higher, you may need a short loading phase prescribed by a clinician.
Should I take vitamin D3 K2 with food or on an empty stomach?
Take it with a meal that contains fat. Vitamins D and K are fat-soluble, and absorption is meaningfully better with dietary fat than on an empty stomach.
Can I take vitamin D3 K2 with calcium or magnesium?
Yes. Calcium and magnesium can be taken with this. If you add calcium, keep total daily calcium from food and supplements reasonable and monitor calcium labs if you have a stone or high-calcium history.
Is vitamin K2 safe if I’m on blood thinners?
Not with warfarin-type blood thinners unless managed by your prescriber. Vitamin K reduces warfarin’s effect and alters INR. Direct oral anticoagulants are less affected, but discuss any vitamin K supplement with your clinician.
What’s the difference between K1 and K2 here?
K1 mainly comes from leafy greens and supports clotting protein activation. K2 (MK-4 in this formula) more strongly activates bone and artery proteins like osteocalcin and matrix Gla protein involved in calcium placement.
Is the vitamin A in this safe for pregnancy?
This uses beta-carotene, a precursor your body converts to vitamin A as needed, unlike preformed retinol that can be risky at high doses. It’s generally acceptable, but confirm total prenatal vitamin A intake with your obstetric clinician.
How to take it & ingredients
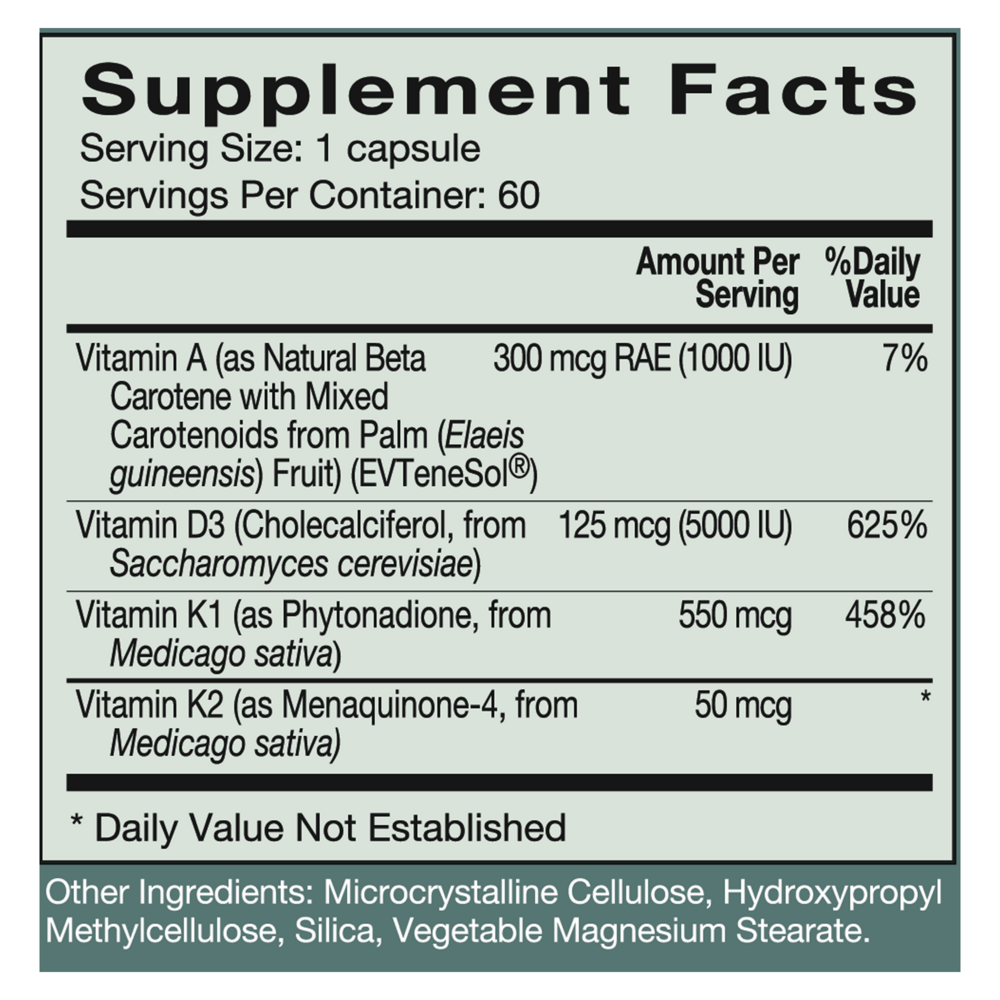
Suggested use: 1 capsule daily or as directed by your healthcare practitioner.
Active ingredients
1 capsule per serving · 60 servings
Vitamin A
As Natural Beta Carotene with Mixed Carotenoids from Palm (Elaeis guineensis) Fruit (EVTeneSol®)
As Natural Beta Carotene with Mixed Carotenoids from Palm (Elaeis guineensis) Fruit (EVTeneSol®)
300 mcg RAE
Vitamin D3
Cholecalciferol, from Saccharomyces cerevisiae
Cholecalciferol, from Saccharomyces cerevisiae
125 mcg
Vitamin K1
As Phytonadione, from Medicago sativa
As Phytonadione, from Medicago sativa
550 mcg
Vitamin K2
As Menaquinone-4, from Medicago sativa
As Menaquinone-4, from Medicago sativa
50 mcg
Other ingredients: Microcrystalline Cellulose, Hydroxypropyl Methylcellulose, Silica, Vegetable Magnesium Stearate
Certifications
Benefits
Warnings
Customers also considered

Bone Restore Calcium Supplement with Vitamin K2
Life Extension
120 capsules
$24.99Save 20% with Subscribe & Save

K-FORCE
Ortho Molecular Products
60 capsules
$60.33Save 10% with Subscribe & Save

K-FORCE MAX
Ortho Molecular Products
30 capsules
$44.79Save 10% with Subscribe & Save

Liquid Vitamin D3 with K2
Ortho Molecular Products
30 milliliters
$52.00Save 10% with Subscribe & Save