

Ortho Molecular Products
Bergamot BPF 1 g by Ortho Molecular Products
60 capsules · 30-day supply
Supports Heart Health and Healthy Cholesterol Levels with Bergamot Extract$66.66
Purchase options
Practitioner-grade brand3rd-party testedFree shipping $50+
Vegan·Vegetarian·Gluten Free·Artificial Color Free·Artificial Flavor Free
Ortho Molecular Products Bergamot BPF overview
If your LDL-C (the cholesterol carried on LDL particles) or ApoB (the count of atherogenic particles) runs high, bergamot extract is worth considering. It also fits adults with elevated Triglycerides, non-HDL-C, or signs of metabolic syndrome, especially when diet and exercise left a residual gap. I reach for it in statin-intolerant patients or as an add-on when LDL-C is still above goal on a moderate statin. Track changes over 4 to 12 weeks with a lipid panel and, when possible, ApoB.
Bergamot extract concentrates citrus polyphenols like brutieridin and melitidin that act on HMG-CoA reductase (the liver enzyme that makes cholesterol), similar in direction to a statin but milder. It also activates AMPK (a cellular energy sensor), which improves how the liver handles fat and reduces VLDL particles (the form your liver packages fat into for transport). Trials show reductions in LDL-C and non-HDL-C, with modest drops in Triglycerides and small improvements in hs-CRP (an inflammation marker) in some responders.
The usual studied amount is 500–1,000 mg of bergamot polyphenolic fraction daily. This formula provides 1 g of bergamot orange extract across 2 capsules; take them together with a meal to limit stomach upset. Expect lipid changes within 4 to 12 weeks. If you need larger LDL-C reductions, bergamot can pair with ezetimibe or a statin, but dose changes belong with your clinician. Recheck a lipid panel, ApoB, and, if elevated at baseline, hs-CRP after 8–12 weeks.
Bergamot and grapefruit share furanocoumarins that can inhibit CYP3A4 (a liver enzyme that clears many drugs). Most bergamot extracts are lower in these, but if you take CYP3A4-cleared medications—like certain calcium channel blockers, immunosuppressants, or statins—loop in your prescriber and start low. Combining with a statin can be effective; watch for new muscle aches. People on diabetes drugs should monitor glucose, as bergamot can nudge it lower. Skip in pregnancy and while breastfeeding due to limited safety data.
Frequently asked questions
Does bergamot really lower cholesterol?
Yes, human trials show bergamot extract lowers LDL-C and non-HDL-C, with modest triglyceride reductions. Effects are milder than high-intensity statins but meaningful for statin-intolerant patients or as an add-on to improve residual risk.
How long does bergamot take to work?
Most lipid changes appear within 4 to 12 weeks. Recheck a lipid panel, ApoB, and, if relevant, hs-CRP after 8–12 weeks to confirm response and adjust the plan.
Can I take bergamot with a statin?
Often, yes. Clinicians use bergamot alongside a statin to further lower LDL-C or allow a lower statin dose. Because both act on liver cholesterol pathways, report new muscle aches and coordinate with your prescriber.
Is bergamot the same as grapefruit for drug interactions?
They’re related. Both contain furanocoumarins that can inhibit CYP3A4, but many bergamot extracts are processed to be lower in these. If you take CYP3A4-metabolized drugs, clear it with your clinician first.
What dose of bergamot should I take?
Most studies use 500–1,000 mg of bergamot polyphenolic fraction daily. This product delivers 1 g per day in two capsules. Take with food to minimize stomach upset.
Will bergamot lower my triglycerides?
It can, but the effect is usually modest. Expect larger LDL-C and non-HDL-C drops, with smaller triglyceride changes. For high triglycerides, pair lifestyle changes with omega-3 or medication if needed.
Are there side effects with bergamot?
It’s generally well tolerated. Occasional issues include mild GI upset, heartburn, or headaches. Rarely, people on statins report muscle aches. Stop and speak with your clinician if symptoms persist.
Who should avoid bergamot?
Avoid in pregnancy and breastfeeding. Use caution if you take CYP3A4-cleared drugs or have significant liver disease. People on diabetes medications should monitor glucose more closely.
How to take it & ingredients
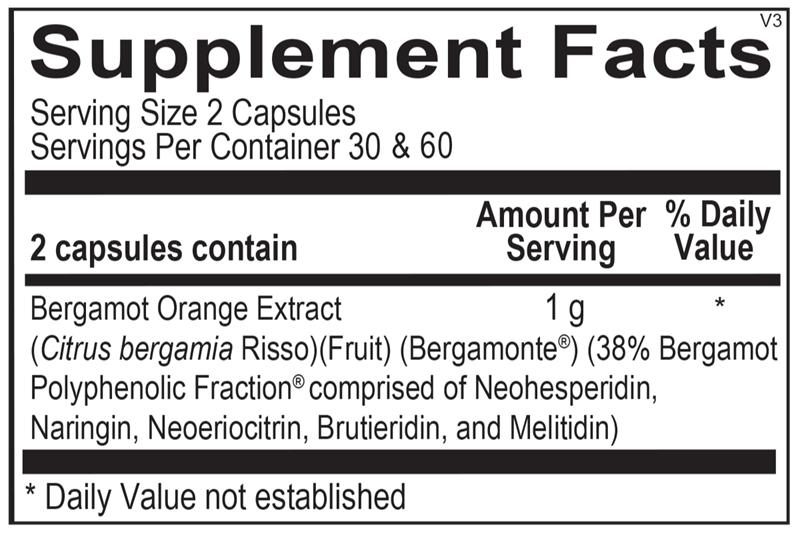
Suggested use: 2 capsules per day or as recommended by your health care professional.
Active ingredients
2 capsules per serving · 30 servings
Bergamot Oragne Extract
Citrus bergamia Risso
Citrus bergamia Risso
1 g
Other ingredients: Natural Vegetable Capsules, Magnesium Stearate, Stearic Acid, Silicon Dioxide
Certifications
Benefits
Warnings
