

Ortho Molecular Products
Cardio B by Ortho Molecular Products
120 capsules · 120-day supply
Comprehensive Methylation Support for Heart and Overall Wellness$73.09
Purchase options
Practitioner-grade brand3rd-party testedFree shipping $50+
Gluten Free·Corn Free·Yeast Free·Artificial Color Free·Artificial Flavor Free
Ortho Molecular Products Cardio B overview
This is for adults with elevated Homocysteine on labs or a family history of early heart disease who want a targeted homocysteine supplement, not a generic multivitamin. It also fits vegans and older adults with low Vitamin B12 or borderline Folate, and people on oral contraceptives or frequent pain relievers who tend to run low on B vitamins. If your homocysteine is normal, you likely do not need this dose.
Homocysteine is a sulfur amino acid your body must recycle. Folate and Vitamin B12 remethylate homocysteine back to methionine (a building-block amino acid), while Vitamin B6 helps convert homocysteine down the detox pathway to cysteine. Betaine (trimethylglycine) donates methyl groups (one-carbon units) as a backup route in the liver. Together, these steps commonly lower homocysteine 20–30% within 4 to 8 weeks if your levels are high at baseline.
Take 1 capsule daily with food, preferably in the morning since B vitamins can feel energizing. Recheck Homocysteine after 4 to 8 weeks to see if you are a responder. If your Vitamin B12 or Folate are low, consider testing Vitamin B12, Methylmalonic Acid (a functional B12 marker), and Folate, RBC, then adjust dosing with your clinician.
This uses high-dose folic acid. People with MTHFR variants sometimes prefer L‑methylfolate; folic acid can still lower homocysteine, but switching forms is reasonable if levels do not budge. Avoid in pregnancy or while trying to conceive unless a clinician recommends this dose. If you have active cancer, take methotrexate for cancer, or recurrent high LDL on betaine, discuss with your doctor first.
Folic acid can reduce side effects of low-dose methotrexate used for autoimmune disease, but high doses should be coordinated with your prescriber. Rarely, betaine can nudge LDL-C up; check a lipid panel (LDL-C or ApoB) after 8 to 12 weeks. Very high chronic B6 can cause nerve symptoms; 50 mg is below typical risk, but report new numbness or tingling.
Frequently asked questions
Will this actually lower my homocysteine?
Often yes. In people with elevated Homocysteine and low-normal B vitamin status, folate, B12, B6, and betaine commonly reduce levels by 20–30% within 4–8 weeks. Recheck the lab to confirm. If it does not move, consider L-methylfolate, higher betaine, or looking for thyroid, kidney, or lifestyle drivers.
Is folic acid or methylfolate better if I have MTHFR?
Both can lower homocysteine. Some with MTHFR variants prefer L-methylfolate because it is the active form. If your Homocysteine falls with folic acid, you’re likely fine. If it stays high or you feel unwell on folic acid, discuss switching to L-methylfolate with your clinician.
When should I take these B vitamins, morning or night?
Morning with food is best. B vitamins can feel stimulating for some people, so taking them earlier reduces sleep disruption. Food improves tolerance if you’re sensitive. Consistency matters more than timing; pick a time you can keep daily.
Is B6 50 mg safe to take long term?
For most adults, 50 mg daily is tolerated. Nerve symptoms have been reported with much higher intakes or multiple B6 sources. If you develop numbness or tingling, stop and speak with your clinician. Periodic breaks or stepping down once Homocysteine normalizes is reasonable.
Can I take this with methotrexate?
Coordinate with your prescriber. Low-dose methotrexate for autoimmune disease is often paired with folic acid on non-methotrexate days. High-dose folate can interfere with methotrexate used for cancer. Do not change folate dosing without medical advice.
Does betaine raise LDL cholesterol?
In a minority of users, betaine can slightly raise LDL-C. If you have a history of high LDL or ApoB, check a lipid panel after 8–12 weeks. If LDL rises meaningfully, you can adjust dose, emphasize diet changes, or use folate/B12/B6 alone.
Is this safe in pregnancy or while trying to conceive?
Not without supervision. This formula contains high-dose folic acid above standard prenatal doses. Use only if your clinician recommends it for a specific reason and monitors your labs.
What labs should I check besides homocysteine?
Consider Vitamin B12, Methylmalonic Acid, and Folate, RBC to see if you’re actually replete. If you’re using betaine and have lipid concerns, recheck a lipid panel (LDL-C or ApoB) after 8–12 weeks.
How to take it & ingredients
Suggested use: 1 or more capsules per day or as recommended by your health care professional.
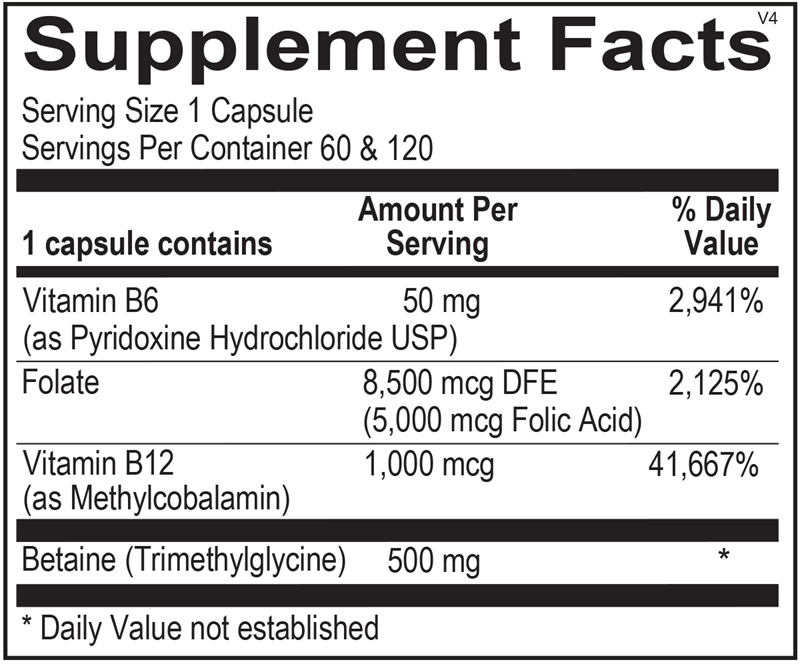
Active ingredients
1 capsule per serving · 120 servings
Vitamin B6
As Pyridoxine Hydrochloride USP
As Pyridoxine Hydrochloride USP
50 mg
Folate
8,500 mcg DFE (5,000 mcg Folic Acid)
8,500 mcg DFE (5,000 mcg Folic Acid)
8500 mcg DFE
Vitamin B12
As Methylcobalamin
As Methylcobalamin
1000 mcg
Betaine
Trimethylglycine
Trimethylglycine
500 mg
Other ingredients: Hypromellose (Natural Vegetable Capsules), Magnesium Stearate
Certifications
Benefits
Warnings