

Ortho Molecular Products
Cardio B by Ortho Molecular Products
60 capsules · 60-day supply
Comprehensive Methylation Support for Heart and Overall Wellness$46.01
Purchase options
Practitioner-grade brand3rd-party testedFree shipping $50+
Gluten Free·Corn Free·Yeast Free·Artificial Color Free·Artificial Flavor Free
Ortho Molecular Products Cardio B overview
If you’re looking for a supplement to lower homocysteine, this B‑complex plus betaine is built for that job. It fits adults whose Homocysteine runs high on labs, especially if Vitamin B12 or Folate are low, or if you have an MTHFR gene variant and don’t eat much leafy greens or animal foods. Vegans, long‑term metformin or acid‑reducing drug users (both can lower B12), and oral‑contraceptive users often land here. Recheck Homocysteine after 6–8 weeks to see if one capsule is enough.
Homocysteine is an amino acid byproduct your body needs to recycle. Folic acid and vitamin B12 donate “methyl” tags (small chemical add‑ons) that convert homocysteine back to methionine, while vitamin B6 helps route it toward cysteine. Betaine (trimethylglycine, or TMG) provides a parallel methyl path in the liver that does not rely on folate activation. In practice, this combo drops Homocysteine about 15–30% within 4–8 weeks in most responders. It lowers the marker reliably, though outcome trials show mixed effects on heart events.
Start with one capsule in the morning with food to limit nausea; B12 can feel energizing if taken late. The label allows one or more daily—many clinicians titrate to two if Homocysteine stays high. Check Vitamin B12 or MMA (methylmalonic acid, a functional B12 marker) if you have neurologic symptoms or follow a vegan diet. Re-test Homocysteine in 6–8 weeks and adjust with your clinician.
If you’re on methotrexate for cancer, do not add folic acid without your oncologist. For low‑dose methotrexate used in arthritis, folate is usually co‑prescribed—coordinate dosing. Very high folate can mask blood signs of B12 deficiency, so correct B12 first if your level or MMA suggests deficiency. Pregnancy requires tailored folate dosing; use only under prenatal guidance. If you’ve had unexplained neuropathy, keep vitamin B6 at or below current dosing.
Frequently asked questions
How long does it take to lower homocysteine?
Most see a homocysteine drop within 4–8 weeks. Take it daily, then recheck Homocysteine on labs. If the number barely moves, your clinician may increase the dose or look for causes like low B12, low kidney function, or hypothyroidism.
Is folic acid or methylfolate better if I have an MTHFR variant?
Both lower homocysteine. High-dose folic acid still works in most people, even with MTHFR variants. Some prefer L‑methylfolate if they’ve had side effects on folic acid. The parallel betaine route here also helps regardless of MTHFR status.
Does lowering homocysteine prevent heart disease?
Lowering the lab number is reliable, but large trials haven’t consistently reduced heart attacks or strokes just by lowering homocysteine. Treat it as risk optimization alongside lipids, blood pressure, smoking, and exercise—then follow outcomes.
Can I take this with metformin or a proton pump inhibitor?
Yes, and it can be useful because both can lower B12 over time. It’s still smart to test Vitamin B12 or MMA yearly if you use those drugs long term, and adjust dosing with your clinician.
What side effects should I watch for?
Occasional nausea or stomach upset, and rare jitteriness from betaine if taken late. Take with food and in the morning. Tingling or numbness is uncommon at this B6 dose; if it appears, stop and speak with your clinician.
Can I take it with aspirin, statins, or blood thinners?
Generally yes—these vitamins and betaine don’t thin blood. If you’re on warfarin or chemotherapy, confirm with your prescriber because folate can interact with some regimens.
Do I still need B12 shots if I use this?
If you have true B12 malabsorption (like pernicious anemia), oral B12 may not be enough. In that case, injections or very high‑dose oral B12 are used. Check Vitamin B12 or MMA to guide the route and dose.
How to take it & ingredients
Suggested use: 1 or more capsules per day or as recommended by your health care professional.
Active ingredients
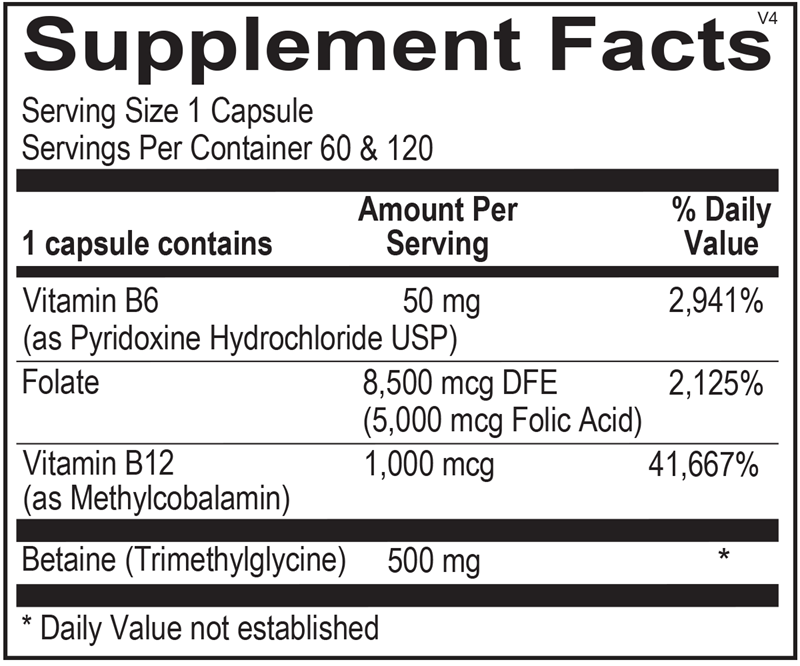
1 capsule per serving · 60 servings
Vitamin B6
As Pyridoxine Hydrochloride USP
As Pyridoxine Hydrochloride USP
50 mg
Folate
8,500 mcg DFE (5,000 mcg Folic Acid)
8,500 mcg DFE (5,000 mcg Folic Acid)
8500 mcg DFE
Vitamin B12
As Methylcobalamin
As Methylcobalamin
1000 mcg
Betaine
Trimethylglycine
Trimethylglycine
500 mg
Other ingredients: Hypromellose (Natural Vegetable Capsules), Magnesium Stearate
Certifications
Benefits
Warnings