

Ortho Molecular Products
Methyl B Complex by Ortho Molecular Products
120 capsules · 120-day supply
Comprehensive B Vitamin Support for Energy and Cognitive Function$54.89
Purchase options
Practitioner-grade brand3rd-party testedFree shipping $50+
Vegetarian·Gluten Free·Corn Free·Yeast Free·Artificial Color Free·Artificial Flavor Free
Ortho Molecular Products Methyl B Complex overview
This is a fit if you’re looking for a methylated B complex because your Homocysteine is high, your Vitamin B12 or Folate is low, or your MCV (red cell size on a CBC) runs high. It’s practical for vegans, metformin users, and people on acid-suppressing drugs who often show low B12 on labs. Those with MTHFR variants who don’t process folic acid well tend to do better with 5‑MTHF and methylcobalamin. If you’re pregnant, use a prenatal formula and clinician guidance.
B vitamins are coenzymes, the helper molecules your enzymes need to turn carbs and fat into ATP (cell energy). 5-MTHF (the active folate) and methylcobalamin (active B12) recycle homocysteine back to methionine, supporting methylation (the on/off tagging of DNA and proteins). Riboflavin (B2) is a cofactor for the MTHFR enzyme, and niacinamide (B3) builds NAD+, the cell’s energy currency. In responders, homocysteine typically drops over 4–12 weeks, and fatigue related to low B status may improve sooner.
Start with one capsule in the morning with food to minimize nausea and jitteriness. Sensitive to methyl donors? Begin every other day for a week, then move to daily as tolerated. The 50 mg B1/B2/B6 and 500 mcg B12 here are potent; if you already take a multivitamin, avoid stacking high-dose Bs. Recheck Vitamin B12, Folate, and Homocysteine after 8–12 weeks to right-size your ongoing dose.
Long-term B6 above typical intakes can cause nerve symptoms; this formula is 50 mg per capsule, so avoid taking multiple daily long term and check Vitamin B6 if you develop tingling. Folate can improve blood counts while a B12 deficiency persists, so pair 5-MTHF with B12 and confirm with MMA (Methylmalonic Acid) or B12 labs. Metformin and proton pump inhibitors commonly lower B12; this B complex can help, but still test. Avoid high-dose folate with methotrexate or similar antifolate drugs unless your clinician directs. Large biotin doses can skew lab tests; the 75 mcg here is small, but still tell your lab about any biotin use.
Frequently asked questions
What does a methylated B complex do?
It provides active forms of folate (5-MTHF) and B12 (methylcobalamin) that your body can use directly. Together with other B vitamins, they help convert food to energy and lower homocysteine, a marker tied to cardiovascular and cognitive risk, over 4–12 weeks.
How long until I feel more energy from B complex?
If low B status is part of your fatigue, people often notice steadier energy within 1–2 weeks. Measurable changes, like lower homocysteine or improved B12 and Folate labs, usually show up after 4–12 weeks of daily use.
Can I take B complex at night?
You can, but it’s more likely to feel stimulating late in the day. Morning with food is the safer bet. If you’re very sensitive to methylated vitamins, start with every other day and move to daily once you know how you respond.
Is methylated B complex better if I have an MTHFR variant?
Often yes. 5-MTHF bypasses the MTHFR step, and riboflavin supports that enzyme. Many with MTHFR variants tolerate 5-MTHF and methylcobalamin better than folic acid and cyanocobalamin, especially when homocysteine is elevated.
Can folate hide a B12 deficiency?
Folate can normalize blood counts while nerve-related B12 deficiency continues. That’s why pairing folate with B12 is standard, and why confirming with Vitamin B12 and MMA (Methylmalonic Acid) testing is smart if you have symptoms or risk factors.
Can B6 in a B complex cause neuropathy?
Very high or prolonged dosing of B6 can cause tingling or numbness. This formula has 50 mg per capsule, which is potent. Avoid taking multiple capsules long term and see your clinician if you develop nerve symptoms.
Do biotin or B vitamins mess up lab tests?
High-dose biotin can interfere with some immunoassays, including thyroid and troponin. The 75 mcg here is low, but still tell your lab you take biotin. Routine B vitamins don’t meaningfully skew standard chemistry or blood counts.
Is this safe with metformin or acid blockers?
Yes, and it’s often useful because both metformin and proton pump inhibitors reduce B12 absorption. Keep using your medications, take the B complex with food, and recheck Vitamin B12 and Homocysteine after 8–12 weeks.
How to take it & ingredients
Suggested use: Take 1 or more capsules per day or as recommended by your health care professional.
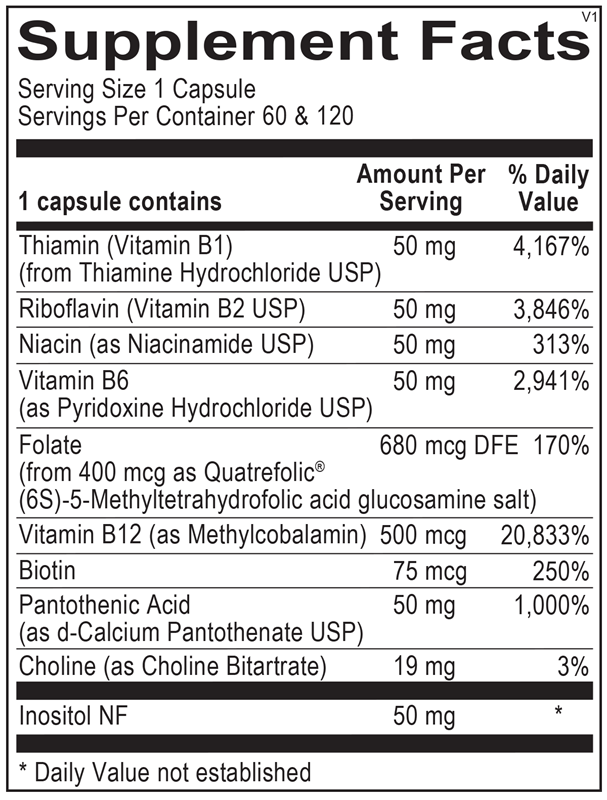
Active ingredients
1 capsule per serving · 120 servings
Thiamin
Thiamine Hydrochloride USP
Thiamine Hydrochloride USP
50 mg
Riboflavin
Riboflavin USP
Riboflavin USP
50 mg
Niacin
Niacinamide USP
Niacinamide USP
50 mg
Vitamin B6
Pyridoxine Hydrochloride USP
Pyridoxine Hydrochloride USP
50 mg
Folate
Quatrefolic® (6S)-5-Methyltetrahydrofolic acid glucosamine salt
Quatrefolic® (6S)-5-Methyltetrahydrofolic acid glucosamine salt
680 mcg DFE
Vitamin B12
Methylcobalamin
Methylcobalamin
500 mcg
Biotin
75 mcg
Pantothenic Acid
D-Calcium Pantothenate USP
D-Calcium Pantothenate USP
50 mg
Inositol
50 mg
Choline
Choline Bitartrate
Choline Bitartrate
19 mg
Other ingredients: Natural Vegetable Capsules, Magnesium Stearate, Silicon Dioxide
Certifications
Benefits
Warnings
Customers also considered

Integrative Therapeutics
Active B-Complex
60 capsules
$18.99extra 21% off with Subscribe & Save

Thorne
B-Complex #12
60 capsules
$26.00extra 10% off with Subscribe & Save

Thorne
B-Complex #6
60 capsules
$26.00extra 10% off with Subscribe & Save

Jarrow Formulas
B-Right
100 capsules
$33.99extra 21% off with Subscribe & Save