

Ortho Molecular Products
Methyl B Complex by Ortho Molecular Products
60 capsules · 60-day supply
Comprehensive B Vitamin Support for Energy and Metabolism$36.24
Purchase options
Practitioner-grade brand3rd-party testedFree shipping $50+
Vegetarian·Gluten Free·Corn Free·Yeast Free·Artificial Color Free·Artificial Flavor Free
Ortho Molecular Products Methyl B Complex overview
This fits people with low energy or brain fog whose Vitamin B12, Folate, or Homocysteine labs are off, and those with a family MTHFR variant. Vegans and vegetarians, metformin or acid-reducer users, and heavy drinkers are common low-B12 or low-B1 cases. If your Methylmalonic Acid (a sensitive B12 status marker) is high or Homocysteine (a byproduct tied to methylation and blood vessel health) is elevated, a methyl B complex is a practical first move. If you’re planning pregnancy, use a dedicated prenatal instead.
This formula uses methylfolate (the active folate form) and methylcobalamin (an active B12) to bypass common genetic bottlenecks in folate/B12 metabolism. Together they recycle homocysteine back to methionine, restoring the cell’s methylation supply (the on–off tags that regulate genes and neurotransmitters). The 50 mg of thiamin, riboflavin, niacinamide, B6, and pantothenate provide the coenzymes your mitochondria use to turn carbs and fats into ATP, which is why fatigue from low B status often improves. Inositol and choline support membrane and neurotransmitter synthesis.
Take one capsule with breakfast to minimize nausea and avoid late-day restlessness. Water-soluble B’s don’t need fat, and bright yellow urine is normal from riboflavin. If your labs are meaningfully low, your clinician may use one to two capsules daily for 4–8 weeks, then step down. Recheck Vitamin B12, Folate, Homocysteine, and Methylmalonic Acid within 8–12 weeks to confirm response.
Folate can correct anemia while a B12-related nerve problem continues, so confirm B12 status if you have numbness or tingling before long-term folate use. Talk to your prescriber if you take methotrexate, anti-seizure drugs (valproate, carbamazepine), or levodopa without carbidopa. High-dose B6 over time can cause neuropathy; the 50 mg here is within typical clinical use. For bipolar disorder, high-dose methylfolate can provoke agitation; use clinician guidance.
Frequently asked questions
What does a methyl B complex do?
It supplies active folate (methylfolate) and B12 (methylcobalamin) plus core B coenzymes. That combination lowers homocysteine, improves cellular energy production, and supports neurotransmitter synthesis when you’re low.
How long until I feel a difference from methyl B vitamins?
Energy and mood changes, if you were low, often show within 1–3 weeks. Homocysteine and Methylmalonic Acid typically improve over 4–8 weeks. If nothing changes by 8–12 weeks, retest and reassess dose or diagnosis.
Can I take a methyl B complex at night?
You can, but morning is better. B vitamins can feel stimulating for some people. If you notice restlessness or vivid dreams, move the dose to breakfast or lunch.
Will methyl B complex cause a niacin flush?
No. This uses niacinamide, a non-flushing form of vitamin B3. You still get B3’s coenzyme benefits without the skin warmth and redness associated with nicotinic acid.
Is methyl B complex safe with metformin or PPIs?
Yes, and it’s often helpful. Metformin and acid reducers are linked with lower B12. Still, check Vitamin B12 and Methylmalonic Acid before and after 8–12 weeks to confirm repletion.
Do I need labs before starting a B-complex?
Not strictly, but it’s smart. Vitamin B12, Folate, Homocysteine, and Methylmalonic Acid baseline values help tailor dose and provide a comparison when you recheck in 8–12 weeks.
Can folate in a B-complex hide a B12 deficiency?
It can correct anemia signs while nerve damage from low B12 continues. If you have numbness or tingling, test Vitamin B12 and Methylmalonic Acid and treat B12 directly.
Is methyl B complex okay in pregnancy?
Use a prenatal instead. Prenatals balance folate, iodine, choline, iron, and other nutrients for pregnancy needs. Ask your obstetric clinician before adding extra B vitamins.
How to take it & ingredients
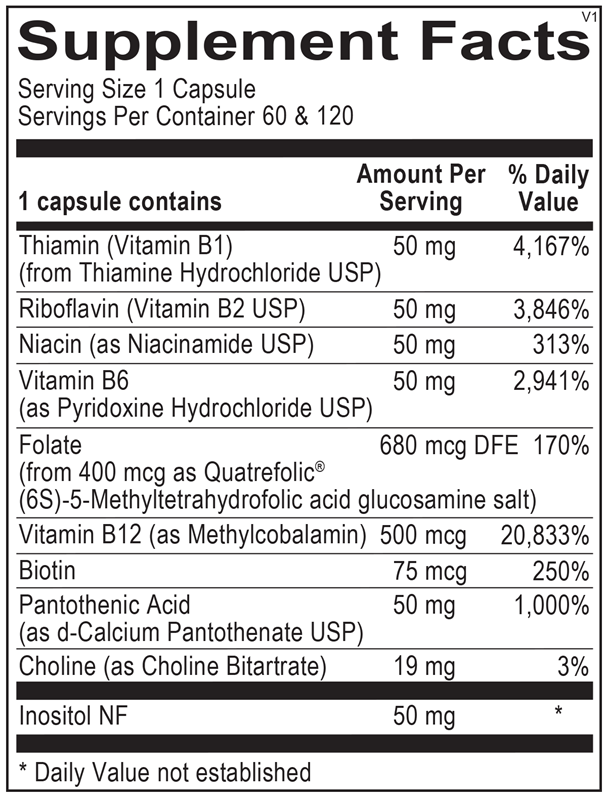
Suggested use: Take 1 or more capsules per day or as recommended by your health care professional.
Active ingredients
1 capsule per serving · 60 servings
Thiamin
Thiamine Hydrochloride USP
Thiamine Hydrochloride USP
50 mg
Riboflavin
Riboflavin USP
Riboflavin USP
50 mg
Niacin
Niacinamide USP
Niacinamide USP
50 mg
Vitamin B6
Pyridoxine Hydrochloride USP
Pyridoxine Hydrochloride USP
50 mg
Folate
Quatrefolic® (6S)-5-Methyltetrahydrofolic acid glucosamine salt
Quatrefolic® (6S)-5-Methyltetrahydrofolic acid glucosamine salt
680 mcg DFE
Vitamin B12
Methylcobalamin
Methylcobalamin
500 mcg
Biotin
75 mcg
Pantothenic Acid
D-Calcium Pantothenate USP
D-Calcium Pantothenate USP
50 mg
Inositol
50 mg
Choline
Choline Bitartrate
Choline Bitartrate
19 mg
Other ingredients: Natural Vegetable Capsules, Magnesium Stearate, Silicon Dioxide
Certifications
Benefits
Warnings
Customers also considered

Integrative Therapeutics
Active B-Complex
60 capsules
$18.99extra 21% off with Subscribe & Save

Thorne
B-Complex #12
60 capsules
$26.00extra 10% off with Subscribe & Save

Thorne
B-Complex #6
60 capsules
$26.00extra 10% off with Subscribe & Save

Jarrow Formulas
B-Right
100 capsules
$33.99extra 21% off with Subscribe & Save