

Ortho Molecular Products
Natural Vitamin E Mixed Tocopherols by Ortho Molecular Products
120 capsules · 60-day supply
Powerful Antioxidant Support for Heart, Skin, and Overall Wellness$85.19
Purchase options
Practitioner-grade brand3rd-party testedFree shipping $50+
Gluten Free·Corn Free·Yeast Free·Artificial Color Free·Artificial Flavor Free
Ortho Molecular Products Natural Vitamin E Mixed Tocopherols overview
This is for adults who want vitamin E as mixed tocopherols vitamin E rather than just alpha-tocopherol. It fits if your Vitamin E (alpha-tocopherol on a blood test) is low or low-normal, if you eat a very low‑fat diet, or have fat malabsorption after bariatric surgery or with long-term orlistat (the fat-blocking drug) or cholestyramine (a bile acid binder). Some clinicians also use high-dose vitamin E in biopsy-proven fatty liver; that should be guided by your doctor with ALT monitoring.
Vitamin E is a family of fat‑soluble antioxidants that sit in cell and LDL membranes and intercept free radicals before they damage fats and proteins. Alpha-tocopherol is the main circulating form, but gamma-tocopherol is common in foods and better at trapping reactive nitrogen species (a form of oxidative stress). High-dose alpha alone can lower gamma levels; a mixed tocopherols vitamin E keeps the family in balance. Expect small, not dramatic, changes in hs-CRP (an inflammation marker) in responders.
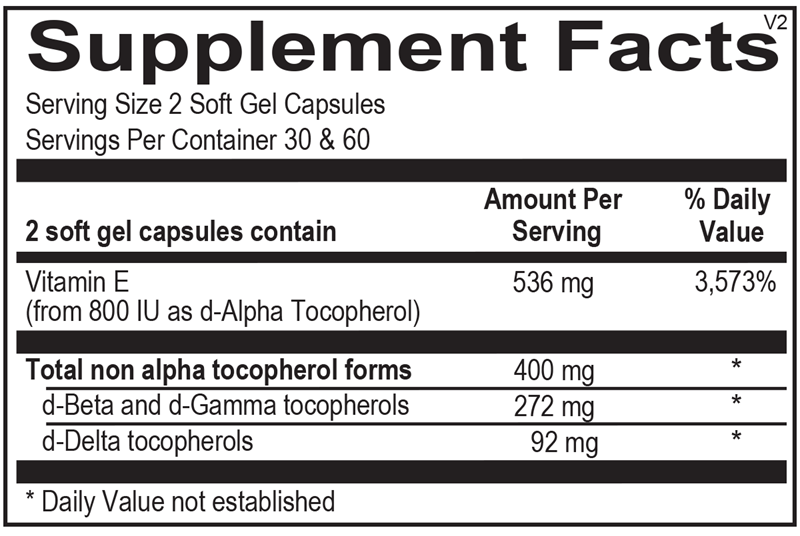
Take 1 softgel daily with a meal that contains fat for absorption; some patients use 2 daily under clinician guidance. The label here supplies about 800 IU natural d‑alpha-tocopherol (536 mg) plus 400 mg of non‑alpha tocopherols per serving, which is a high dose. For simple maintenance when your level isn’t low, a lower‑dose vitamin E is usually sufficient.
If you use warfarin, apixaban, rivaroxaban, clopidogrel, or daily aspirin, high-dose vitamin E can increase bleeding risk; involve your clinician and monitor. Hold 1 week before elective surgery. The SELECT trial linked 400 IU/day synthetic alpha-tocopherol to higher prostate cancer risk in men; that argues against casual long-term high-dose use. Avoid in unexplained vitamin K deficiency. Pregnancy: ask your OB before using doses above prenatal multivitamin levels.
Frequently asked questions
Is mixed tocopherols better than alpha-tocopherol?
For most people, yes. Mixed tocopherols preserve gamma-tocopherol, which high-dose alpha alone can suppress. Gamma handles reactive nitrogen species well. If you supplement, using a mix mirrors diet better than alpha-only.
How long does vitamin E take to work?
Blood alpha-tocopherol typically rises within 2–4 weeks. Clinical outcomes depend on the goal; antioxidant markers and skin dryness often change over weeks, not days. Retest Vitamin E (alpha-tocopherol) after 6–8 weeks if you’re correcting a low level.
Can vitamin E thin your blood?
At higher doses, vitamin E has a mild anti‑platelet effect. Combined with warfarin, apixaban, rivaroxaban, clopidogrel, or daily aspirin, bleeding risk increases. If you’re on these, use lower doses or skip unless your clinician is monitoring you.
Should I take vitamin E with food or on an empty stomach?
Take it with a meal that contains fat. Vitamin E is fat‑soluble, and absorption is significantly better when taken with dietary fat than on an empty stomach.
What labs should I check with vitamin E?
Check Vitamin E (alpha-tocopherol) to document low or low‑normal status and recheck after 6–8 weeks. In specific cases like fatty liver, clinicians may also follow ALT and AST (liver enzymes) while using higher doses.
Is natural vitamin E different from synthetic?
Yes. Natural d‑alpha-tocopherol is better retained than synthetic dl‑alpha. Large trials that suggested harms used synthetic alpha only. Mixed natural tocopherols avoid that imbalance, though high-dose use still warrants caution.
Can smokers take vitamin E?
Vitamin E alone isn’t contraindicated, but avoid beta‑carotene supplements if you smoke. If you’re on blood thinners or have frequent nosebleeds or bruising, discuss vitamin E with your clinician before using higher doses.
How to take it & ingredients
Suggested use: 1-2 soft gel capsules per day or as recommended by your health care professional.
Active ingredients
2 capsules per serving · 60 servings
Vitamin E
From 800 IU as d-Alpha Tocopherol
From 800 IU as d-Alpha Tocopherol
536 mg, 800 IU
▼
Total non-alpha tocopherol forms
400 mg
d-Beta and d-Gamma tocopherols
272 mg
d-Delta tocopherols
92 mg
Certifications
Benefits
Warnings