

Ortho Molecular Products
Natural Vitamin E Mixed Tocopherols by Ortho Molecular Products
60 capsules · 30-day supply
Powerful Antioxidant Support for Heart and Skin Health$52.89
Purchase options
Practitioner-grade brand3rd-party testedFree shipping $50+
Gluten Free·Corn Free·Yeast Free·Artificial Color Free·Artificial Flavor Free
Ortho Molecular Products Natural Vitamin E Mixed Tocopherols overview
This is for people looking for vitamin E mixed tocopherols rather than alpha-only capsules. It fits those with low dietary intake of nuts and seeds, very low–fat diets, or fat-malabsorption (after bariatric surgery, with chronic pancreatitis, celiac disease, cystic fibrosis, or on orlistat, the fat-blocking drug). If your Vitamin E (alpha-tocopherol), serum is low, mixed tocopherols replete and maintain both alpha and gamma forms. For general prevention without deficiency, this dose is often more than you need.
Vitamin E is a family of fat-soluble antioxidants that sit in cell and lipoprotein membranes and neutralize free radicals before they damage fats and proteins. Alpha-tocopherol is best retained in blood, but high alpha alone can lower gamma-tocopherol, the form most common in food. Mixed tocopherols restore that balance. They help limit oxidation of LDL particles (the cholesterol carriers linked to plaque) and reduce lipid peroxidation, which explains small shifts in hs-CRP (a general inflammation marker) in some studies. Large trials have not shown broad heart-disease or cancer prevention from routine high-dose E.
Take 1 softgel daily with a meal that contains fat, and only use 2 daily under clinician guidance. This is a high dose compared with multivitamin levels, intended for repletion or targeted use. Blood levels of alpha-tocopherol respond within 4 to 8 weeks. If you also take fish oil, a combined meal is fine. If your level is significantly low, plan on retesting Vitamin E (alpha-tocopherol), serum after 8 to 12 weeks.
Skip high-dose vitamin E if you take warfarin or other blood thinners, or if you have a bleeding disorder, unless your prescriber agrees and monitors. Use caution with dual antiplatelet therapy (aspirin plus clopidogrel). Do not start around chemotherapy or radiation without oncology input. A past trial linked long-term high-dose alpha-tocopherol to higher prostate cancer risk, so routine use for disease prevention is not advised.
Frequently asked questions
Is mixed tocopherols better than alpha-tocopherol alone?
For most people, yes. Alpha is best retained in blood, but high alpha alone can suppress gamma-tocopherol. Mixed tocopherols provide alpha plus meaningful gamma and delta, closer to food patterns and better for long-term balance.
How long does vitamin E take to raise my levels?
Serum alpha-tocopherol usually rises within 4 to 8 weeks. If you started for a low Vitamin E (alpha-tocopherol), serum, recheck in 8 to 12 weeks and adjust the dose or diet based on results and symptoms.
Does vitamin E thin your blood?
At high doses it can increase bleeding risk, especially with warfarin, aspirin, clopidogrel, or fish oil. If you use blood thinners or have a bleeding history, avoid high-dose vitamin E unless your clinician is monitoring you.
Should I take vitamin E with food or on an empty stomach?
Take it with a meal that contains fat. Vitamin E is fat-soluble, and co-ingestion with dietary fat improves absorption meaningfully compared with taking it on an empty stomach.
Can I take vitamin E with fish oil?
Yes, and taking them with the same meal is convenient. Both are fat-soluble. Just be mindful that combining high-dose vitamin E with higher-dose fish oil can raise bleeding risk if you also use blood thinners.
Who should consider testing vitamin E levels?
Testing is useful if you have fat-malabsorption, unexplained neuropathy, abnormally low cholesterol, very low–fat intake, or long-term orlistat use. Ask for Vitamin E (alpha-tocopherol), serum and reassess after targeted repletion.
Is vitamin E safe during pregnancy?
Avoid high-dose vitamin E in pregnancy unless prescribed. Standard prenatal vitamins already include modest amounts. If deficiency is suspected, work with your obstetric clinician and confirm by lab testing before supplementing.
Will vitamin E help my skin?
Oral vitamin E improves systemic antioxidant status, but evidence for wrinkles or acne is limited. It can help in documented deficiency or severe dryness related to low fat intake. Topical vitamin E is a separate consideration.
How to take it & ingredients
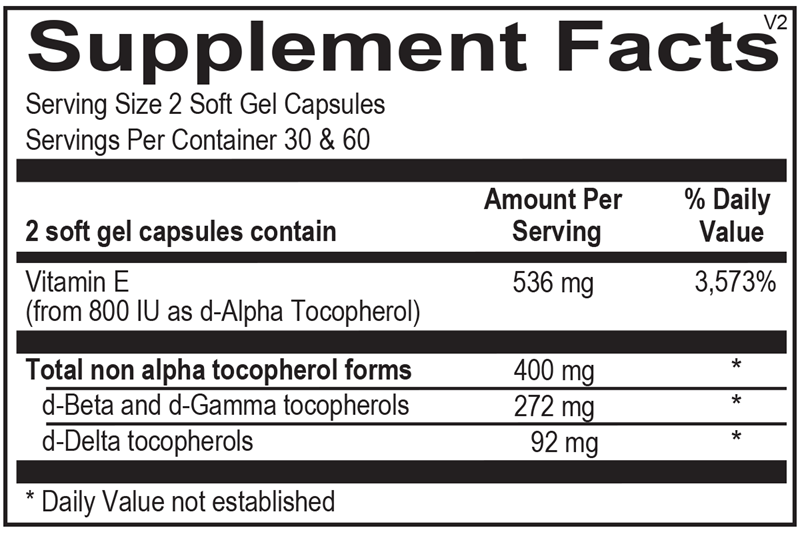
Suggested use: 1-2 soft gel capsules per day or as recommended by your health care professional.
Active ingredients
2 capsules per serving · 30 servings
Vitamin E
From 800 IU as d-Alpha Tocopherol
From 800 IU as d-Alpha Tocopherol
536 mg, 800 IU
▼
Total non-alpha tocopherol forms
400 mg
d-Beta and d-Gamma tocopherols
272 mg
d-Delta tocopherols
92 mg
Certifications
Benefits
Warnings