What is in each capsule?
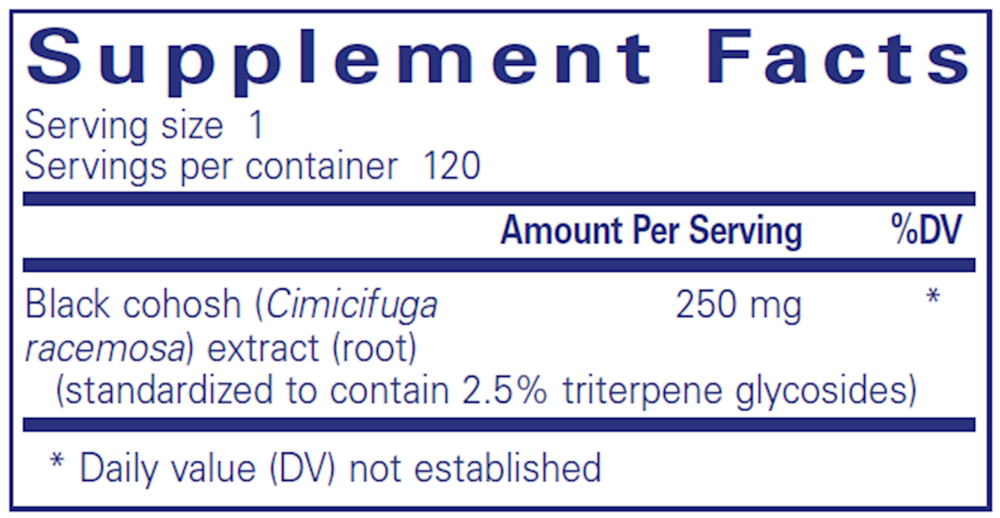
Each capsule contains 250 mg of black cohosh (Cimicifuga racemosa) extract from the root, standardized to contain 2.5 percent triterpene glycosides. It is a single-ingredient formula.
What does the 2.5 in the name mean?
The 2.5 refers to the standardization. The extract is standardized to contain 2.5 percent triterpene glycosides.
What is black cohosh?
Black cohosh (Cimicifuga racemosa) is a plant whose root is used in botanical supplements. This product uses a standardized extract of the root.
How do I take it?
Pure Encapsulations' suggested use is one capsule, one to two times daily, between meals. Follow the dose on the label or the direction of your clinician.
How many capsules are in the bottle?
120 vegetarian capsules. At one capsule per serving, that is 120 servings per container.
Is the capsule vegetarian?
Yes. The capsule is made from cellulose and water. The other ingredient listed is hypoallergenic plant fiber (cellulose). Pure Encapsulations labels the product gluten free, non-GMO, and hypoallergenic and states it is made with vegan ingredients.
How should I store it?
Store at room temperature away from heat and moisture, and keep out of the reach of children.