


Pure Encapsulations
Junior Nutrients by Pure Encapsulations
120 capsules · 60-day supply
Comprehensive Multivitamin for Growing Minds and Bodies$31.50
Purchase options
Practitioner-grade brand3rd-party testedFree shipping $50+
Gluten Free·Egg Free·Artificial Preservative Free·Peanut Free·Wheat Free·Artificial Sweetener Free·
Pure Encapsulations Junior Nutrients overview
Picky eaters, dairy- or egg-free kids, and children who get little sun are the ones who actually benefit from a children's multivitamin. If your child’s Vitamin D, 25-Hydroxy is low, if Ferritin (iron storage) runs low-normal, or if greens and colorful produce are sparse, this fills common gaps. It’s iron-free, so it’s a fit for families who prefer to manage iron separately. For established deficiencies, treat to target first, then use this for maintenance.
This formula uses L-5-MTHF (the folate form the body can use directly) plus methylcobalamin (the active B12) and activated B6 (pyridoxal 5-phosphate) to cover kids who don’t convert these vitamins efficiently. Lutein and zeaxanthin concentrate in the macula (the part of the retina for sharp vision), helpful when leafy greens and egg yolks are low. D3 is the same form your skin makes from sunlight. Gentle mineral forms, like di-magnesium malate and zinc citrate, are easier on the stomach.
Give with food to improve absorption and avoid nausea. Ages 4–13: 2 capsules daily. Ages 14+: 4 capsules daily. Splitting morning and evening with meals works well. Separate from thyroid medication by at least 4 hours, and from antibiotics that bind minerals (tetracyclines, fluoroquinolones) by 2–6 hours. Expect steady changes in Vitamin D, 25-Hydroxy and B-vitamin markers within 4–12 weeks.
Choose a children’s multivitamin with iron if Ferritin is low or your clinician recommends iron; this one is iron-free. If your child takes warfarin (a blood thinner), vitamin K in multis can affect dosing—talk to the prescriber. Avoid stacking extra vitamin A from cod liver oil. Separate calcium/magnesium from levothyroxine and mineral-binding antibiotics as noted. For allergies or special diets, confirm excipients match your needs.
Frequently asked questions
Is this children’s multivitamin iron-free?
Yes. There’s no iron in this formula. That’s helpful if you’re monitoring iron separately or your child doesn’t need extra. If Ferritin is low or your clinician advises iron, pick a multivitamin with iron or add a standalone iron and retest.
Can I open the capsules and mix into food?
Yes. You can open the capsules and mix the powder into a small amount of yogurt, applesauce, or a smoothie. Give with a meal for better absorption and to reduce the chance of mild stomach upset.
How long until a kids multivitamin makes a difference?
Blood markers usually shift within 4–12 weeks. Vitamin D, 25-Hydroxy and B-vitamin status change first, while carotenoids like lutein build gradually in tissues. Energy and appetite are variable and shouldn’t be used alone to judge response.
Is lutein safe for children’s eyes?
Yes. Lutein and zeaxanthin are dietary carotenoids found in greens and eggs, and they accumulate in the macula. The doses here (3 mg lutein, 500 mcg zeaxanthin) are within typical dietary-supplement ranges used in pediatric formulas.
Does vitamin K in a multivitamin affect blood thinners?
It can. Vitamin K can interfere with warfarin dosing. If your child uses warfarin, consult the prescriber before starting and keep vitamin K intake consistent if approved. Direct oral anticoagulants are less affected, but still review with the clinician.
Can my child take this with a separate vitamin D?
Usually yes. This multivitamin provides a modest D3 amount. If Vitamin D, 25-Hydroxy is low, a separate D3 can be layered under clinician guidance, then scaled back once repleted. Recheck levels after 8–12 weeks to avoid overshooting.
What side effects should I watch for?
Mild nausea or a metallic taste from zinc can occur if taken without food. Rarely, loose stools happen with magnesium. Taking with meals and splitting the dose helps. Stop and consult your clinician if you notice rash, persistent stomach pain, or headaches.
How to take it & ingredients
Suggested use: Ages 4 to 13, take 2 capsules daily, with a meal. Ages 14 and up, take 4 capsules daily, with meals.
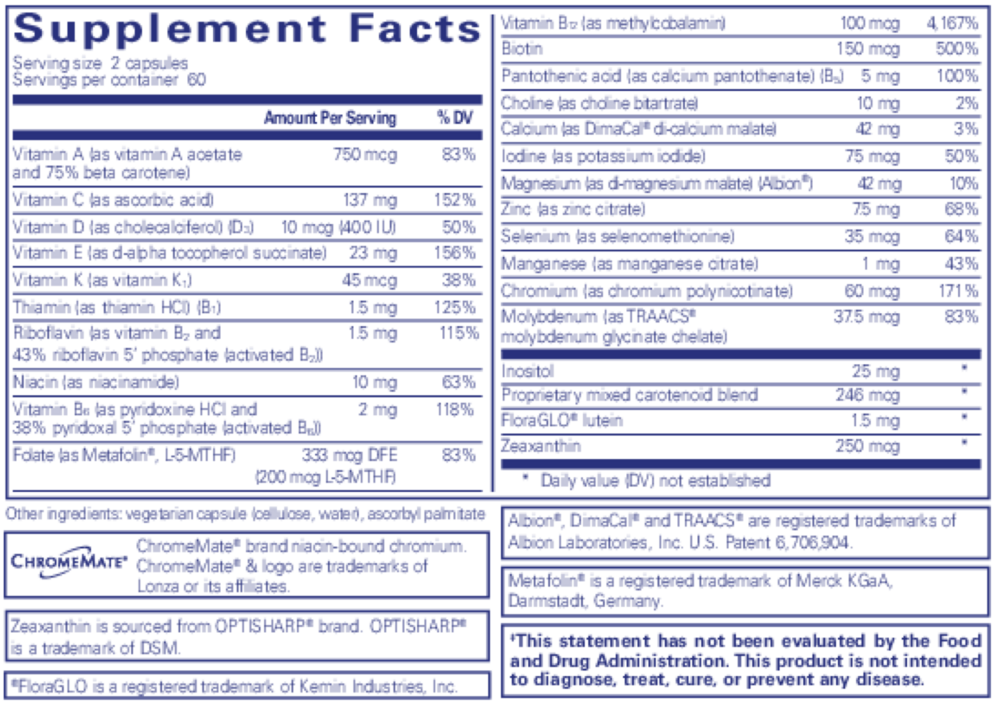
Active ingredients
2 capsules per serving · 60 servings
Vitamin A
As vitamin A acetate and 75% beta carotene
As vitamin A acetate and 75% beta carotene
750 mcg
Vitamin C
As ascorbic acid
As ascorbic acid
137 mg
Vitamin D
As cholecalciferol (D3)
As cholecalciferol (D3)
10 mcg
Vitamin E
As d-alpha tocopherol succinate
As d-alpha tocopherol succinate
23 mg
Vitamin K
As vitamin K1
As vitamin K1
45 mcg
Thiamin
As thiamin HCl (B1)
As thiamin HCl (B1)
1.5 mg
Riboflavin
Vitamin B2
Vitamin B2
1.5 mg
Niacin
As niacinamide
As niacinamide
10 mg
Vitamin B6
As pyridoxine HCl
As pyridoxine HCl
2 mg
Folate
As Metafolin®, L-5-MTHF, 200 mcg L-5-MTHF
As Metafolin®, L-5-MTHF, 200 mcg L-5-MTHF
333 mcg DFE
Vitamin B12
As methylcobalamin
As methylcobalamin
100 mcg
Biotin
150 mcg
Pantothenic Acid
As calcium pantothenate (B5)
As calcium pantothenate (B5)
5 mg
Calcium
As di-calcium malate (DimaCal™)
As di-calcium malate (DimaCal™)
42 mg
Iodine
As potassium iodide
As potassium iodide
75 mcg
Magnesium
As di-magnesium malate (Albion™)
As di-magnesium malate (Albion™)
42 mg
Zinc
As zinc citrate
As zinc citrate
7.5 mg
Selenium
As selenomethionine
As selenomethionine
35 mcg
Manganese
As manganese citrate
As manganese citrate
1 mg
Chromium
As chromium polynicotinate
As chromium polynicotinate
60 mcg
Molybdenum
As TRAACS® molybdenum glycinate chelate
As TRAACS® molybdenum glycinate chelate
37.5 mcg
Riboflavin 5 Phosphate
Activated B2
Activated B2
1.7 mg
Pyridoxal 5 Phosphate
Activated B6
Activated B6
2.5 mg
Choline Bitartrate
50 mg
Inositol
50 mg
Mixed Carotenoids
493 mcg
Lutein
MacularSynergy Complex
MacularSynergy Complex
3 mg
Zeaxanthin
MacularSynergy Complex
MacularSynergy Complex
500 mcg
Other ingredients: ascorbyl palmitate, vegetarian capsule (cellulose, water)
Certifications
Benefits
Warnings
Customers also considered

Now Foods
ADAM Superior Men's Multi
90 softgels
$39.99extra 20% off with Subscribe & Save

Nature's Way
Alive Womens 50+ Premium Gummy Multi-Vitamin
75 gummies
$22.99extra 22% off with Subscribe & Save

Nature’s Way
Alive! Men’s 50+ Ultra Potency
60 tablets
$29.99extra 20% off with Subscribe & Save

Ortho Molecular Products
Alpha Base® Capsules with Iron
240 capsules
$74.31extra 10% off with Subscribe & Save