

Ritual
Essential for Women 50+ Multivitamin by Ritual
60 capsules · 30-day supply
Comprehensive Multivitamin Support for Women Over 50$44.99
Purchase options
Practitioner-grade brand3rd-party testedFree shipping $50+
Vegan·Vegetarian·Gluten Free·Soy Free·Dairy Free·Sugar Free·
Ritual Essential for Women 50+ Multivitamin overview
A multivitamin for women over 50 makes sense if your Vitamin D, 25-Hydroxy runs low, you eat little seafood, or you prefer a vegan option. This formula covers D3, K2, methylfolate, methylcobalamin (B12), magnesium, and algal DHA. It fits post-menopausal adults focused on bone, brain, and heart aging markers. If your Omega-3 Index is low or homocysteine (an amino acid linked to vascular risk) trends high, these specific nutrients are relevant. If your triglycerides are elevated, the DHA here is maintenance-level, not a triglyceride-lowering dose.
Vitamin D3 raises calcium absorption, while K2 as MK-7 activates osteocalcin (a bone protein that helps lock calcium into bone) to direct calcium away from arteries. DHA from microalgae integrates into brain-cell membranes and can nudge down hs-CRP (a general inflammation marker) in some responders. Methylfolate and methylcobalamin lower homocysteine, which is tied to cardiovascular and cognitive aging risk. Mixed tocopherols supply vitamin E beyond just alpha-tocopherol. Dimagnesium malate is a gentle form; the dose supports intake but is not a full repletion strategy.
Take two capsules together once daily, with or without food; a small meal can reduce mild nausea. Consistency matters: plan 4 to 12 weeks to see shifts in Vitamin D, 25-Hydroxy or Omega-3 Index, and about 8 weeks for homocysteine. If you use levothyroxine for thyroid, separate all supplements by at least 4 hours. If you need higher-dose vitamin D or omega-3 based on labs, layer separate D3 or fish/algal oil rather than exceeding the multivitamin serving.
Vitamin K2 interacts with warfarin (the blood thinner that’s vitamin K–sensitive), so skip this or coordinate closely with your prescriber if you use warfarin. K2 does not meaningfully affect newer blood thinners. Use caution if you’ve had high calcium or granulomatous disease like sarcoidosis, where vitamin D needs supervision. With advanced kidney disease, discuss magnesium with your nephrologist. For iron deficiency shown by low Ferritin, this iron-free multivitamin is not sufficient; add iron separately under guidance.
Frequently asked questions
Is algal DHA as effective as fish oil DHA?
Yes. DHA from microalgae is chemically identical to fish-derived DHA and raises the Omega-3 Index similarly. The 330 mg here is a maintenance dose, not a triglyceride-lowering dose. If you need higher omega-3 intake, add a separate algal or fish oil.
How long until I notice benefits from this multivitamin?
Lab shifts usually show first: Vitamin D and Omega-3 Index often change within 4–12 weeks, and homocysteine can drop in about 8 weeks. Symptom changes like steadier energy or fewer leg cramps vary and are not guaranteed.
Does vitamin K2 interfere with blood thinners?
It can with warfarin, which is sensitive to vitamin K and requires stable intake. Do not start this without prescriber approval if you use warfarin. K2 does not meaningfully affect most newer anticoagulants, but still confirm with your clinician.
Does this multivitamin contain iron or calcium?
No iron and no calcium. That suits most post-menopausal adults, who often don’t need routine iron unless Ferritin is low. If your calcium intake is low, use diet or a separate calcium supplement taken with meals.
Can I take this with thyroid medication?
Yes, but separate by at least 4 hours. Minerals and certain vitamins can reduce levothyroxine absorption. Take your thyroid pill on an empty stomach, then take the multivitamin later in the day.
Will DHA or vitamin E thin my blood?
At the amounts here, meaningful bleeding risk is unlikely for most people. The bigger interaction is vitamin K2 with warfarin. If you’re on any anticoagulant or have a bleeding disorder, review the full ingredient list with your clinician.
Is methylfolate better if I have an MTHFR variant?
Methylfolate is the bioactive form and bypasses the MTHFR conversion step. It’s a practical choice if you’ve had low folate status or elevated homocysteine, though routine genetic testing isn’t necessary to benefit.
How to take it & ingredients
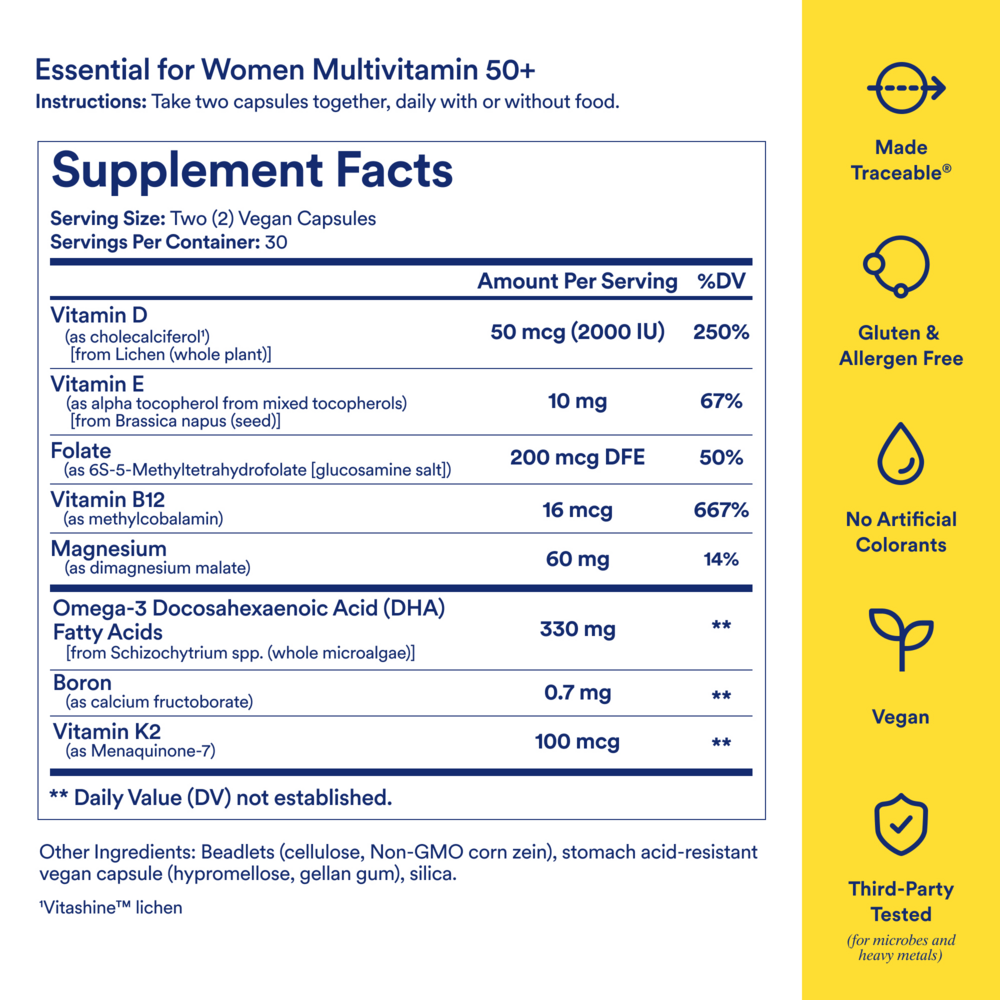
Suggested use: For women 50+. Take two capsules together daily, with or without food. Keep in a cool, dry place, out of direct sunlight.
Active ingredients
2 capsules per serving · 30 servings
Vitamin D
As cholecalciferol, from Lichen (whole plant)
As cholecalciferol, from Lichen (whole plant)
50 mcg
Vitamin E
As alpha-tocopherol from mixed tocopherols, from Brassica napus (seed)
As alpha-tocopherol from mixed tocopherols, from Brassica napus (seed)
10 mg
Folate
As 6S-5-methyltetrahydrofolate (glucosamine salt)
As 6S-5-methyltetrahydrofolate (glucosamine salt)
200 mcg DFE
Vitamin B12
As methylcobalamin
As methylcobalamin
16 mcg
Magnesium
As dimagnesium malate
As dimagnesium malate
60 mg
Omega-3 Docosahexaenoic Acid (DHA) Fatty Acids
From Schizochytrium sp. (whole microalgae)
From Schizochytrium sp. (whole microalgae)
330 mg
Boron
As calcium fructoborate
As calcium fructoborate
0.7 mg
Vitamin K2
As Menaquinone-7
As Menaquinone-7
100 mcg
Other ingredients: Beadlets (Cellulose, Non-GMO Corn Zein), Stomach Acid-Resistant Vegan Capsule (Hypromellose, Gellan Gum), Silica
Certifications
Benefits
Warnings
Customers also considered

ADAM Superior Men's Multi
Now Foods
90 softgels
$39.99Save 20% with Subscribe & Save

Alive Womens 50+ Premium Gummy Multi-Vitamin
Nature's Way
75 gummies
$22.99Save 22% with Subscribe & Save

Alive! Men’s 50+ Ultra Potency
Nature’s Way
60 tablets
$29.99Save 20% with Subscribe & Save

Alpha Base® Capsules with Iron
Ortho Molecular Products
240 capsules
$74.31Save 10% with Subscribe & Save