

Theralogix
TheraLith XR magnesium and potassium citrate, vitamin B6 by Theralogix
360 tablets · 180-day supply
Essential Magnesium & Potassium for Optimal Muscle and Nerve Function$75.99
Purchase options
Practitioner-grade brand3rd-party testedFree shipping $50+
Vegan·Vegetarian·Gluten Free
Theralogix TheraLith XR magnesium and potassium citrate, vitamin B6 overview
If you are prone to calcium oxalate kidney stones and your 24-hour urine shows low citrate (hypocitraturia, meaning not enough citrate to bind calcium) or a low urine pH (more acidic urine), potassium citrate for kidney stones is a practical, gentler option. The extended-release tablets suit people who cannot tolerate prescription doses. This maintenance-level mix also fits high-oxalate eaters, low-carb diets that acidify urine, and post–bariatric surgery patients. If your stones are calcium phosphate with already alkaline urine, you need clinician guidance before adding any alkalinizer.
Potassium citrate raises urinary citrate, which binds calcium to form soluble complexes, and it nudges urine pH upward, making calcium oxalate and uric acid crystals less likely to form. Magnesium (here as oxide and oxide-citrate) can pair with oxalate in the gut and urine, lowering free oxalate available to crystallize. Vitamin B6 (pyridoxine) is a cofactor that can reduce the body’s own oxalate production in some people. On labs, responders see urine citrate and pH improve within 4 to 8 weeks.
Take two tablets with breakfast and two with dinner, with food and plenty of water. This total daily potassium is lower than typical prescription potassium citrate, so think of it as maintenance or as an add-on when partial alkalinization is desired. Recheck a 24-hour urine (citrate, pH, calcium, oxalate, uric acid) after 6 to 8 weeks, and track a Basic Metabolic Panel for potassium and kidney function if you increase dose or combine with other alkalinizers.
Avoid potassium citrate if you have chronic kidney disease or a history of high potassium. Do not combine with potassium-sparing drugs like spironolactone, eplerenone, amiloride, or triamterene, and use caution with ACE inhibitors, ARBs, or aliskiren, which also raise potassium. Separate magnesium from levothyroxine, tetracycline or fluoroquinolone antibiotics, and oral bisphosphonates by 4 hours to avoid absorption issues. If you have recurrent calcium phosphate stones or active urinary infections with alkaline urine, get clinician guidance first.
Frequently asked questions
Does potassium citrate actually prevent kidney stones?
Yes for many calcium oxalate and uric acid stone formers. It raises urine citrate and pH, which makes crystals less likely to form. Effectiveness is best confirmed by a 24-hour urine test showing improved citrate and pH after 4–8 weeks.
Is this dose as strong as prescription potassium citrate?
No. Four tablets provide a lower total potassium than common prescription regimens. It works well for maintenance, intolerance to higher doses, or as an add-on. If your urine citrate is very low or stones are frequent, you may need prescription-strength under medical care.
How long before labs change on potassium citrate?
Most responders see higher urine citrate and a modest rise in urine pH within 4 to 8 weeks. Recheck a 24-hour urine to verify the change and adjust dosing. Stone risk reductions track with those laboratory improvements.
Can I take this with blood pressure medicines like ACE inhibitors or ARBs?
Use caution. ACE inhibitors and ARBs can raise potassium, and adding potassium citrate increases that risk. If used together, you need clinician oversight and periodic Basic Metabolic Panel checks to monitor potassium and kidney function.
Will magnesium and vitamin B6 help with oxalate?
Magnesium can bind oxalate in the gut and urine, lowering free oxalate. Vitamin B6 helps some people make less oxalate. The effects are usually modest but additive with potassium citrate. Verify changes by checking 24-hour urine oxalate.
What side effects should I watch for?
The extended-release tablets are gentler on the stomach, but some people get mild GI upset or loose stools, usually from magnesium. Taking with meals and splitting doses helps. Stop and seek care if you develop muscle weakness, palpitations, or persistent vomiting.
Can potassium citrate help with uric acid stones or gout?
It can. By raising urine pH, potassium citrate helps dissolve and prevent uric acid stones. It is not a gout treatment, but improving urine chemistry reduces uric acid crystallization in the urinary tract.
Do I need to separate this from other medications?
Yes for certain drugs. Take magnesium-containing tablets at least 4 hours apart from levothyroxine, tetracycline or fluoroquinolone antibiotics, and oral bisphosphonates to avoid reduced absorption.
How to take it & ingredients
Suggested use: Take two tablets, twice a day, with meals. For example, take two tablets with breakfast and two tablets with dinner. Do not exceed recommended dosage.
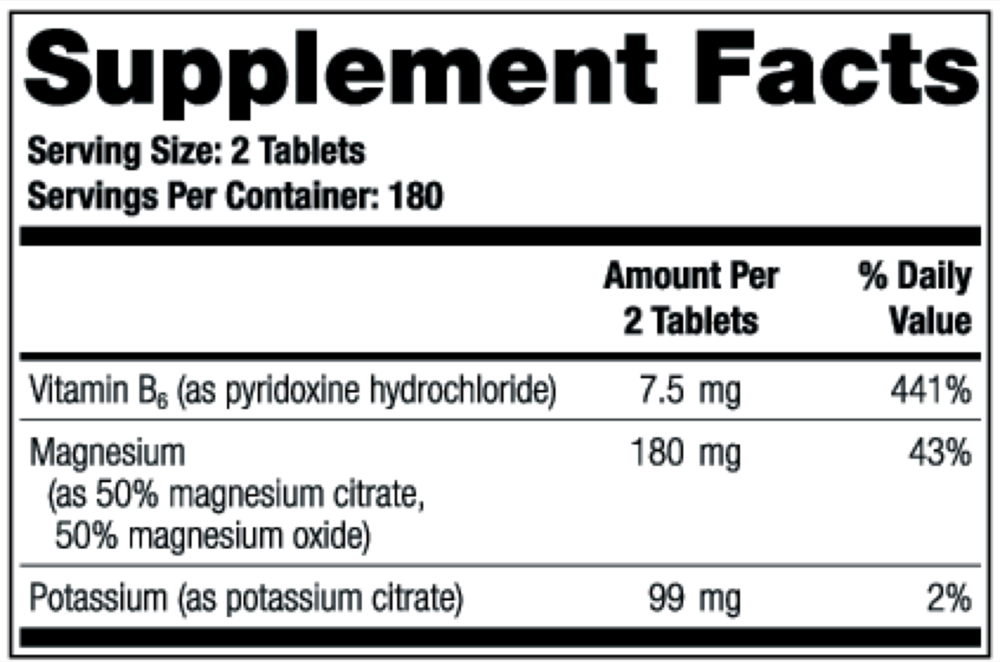
Active ingredients
2 tablets per serving · 180 servings
Vitamin B6
As pyridoxine hydrochloride
As pyridoxine hydrochloride
7.5 mg
Magnesium
As 50% magnesium oxide citrate, 50% magnesium oxide
As 50% magnesium oxide citrate, 50% magnesium oxide
180 mg
Potassium
As potassium citrate
As potassium citrate
99 mg
Other ingredients: Microcrystalline cellulose, Vegetable stearic acid, Vegetable magnesium stearate, Silicon dioxide, White enteric coating (hypromellose, polydextrose, calcium carbonate, medium chain triglycerides, purified water, ethylcellulose, ammonium hydroxide, oleic acid, sodium alginate)
Certifications
Benefits
Warnings
Customers also considered

CereMag
Ortho Molecular Products
99 grams
$77.76Save 10% with Subscribe & Save

Dr. Formulated Magnesium Raspberry
Garden of Life
197.4 grams
$24.99Save 20% with Subscribe & Save

Dual-Mag Complex
Natura Health Products
90 capsules
$22.99Save 22% with Subscribe & Save

Mag Threonate
Ortho Molecular Products
60 capsules
$78.64Save 10% with Subscribe & Save