

Theralogix
TheraNatal Core by Theralogix
90 tablets · 90-day supply
Comprehensive Prenatal Support for Mom and Baby's Health$40.99
Purchase options
Practitioner-grade brand3rd-party testedFree shipping $50+
Vegetarian·Gluten Free
Theralogix TheraNatal Core overview
Planning pregnancy in the next few months is the right time to start a prenatal vitamin for trying to conceive. This formula covers the basics for neural tube formation early in the first trimester, with L‑5‑methyltetrahydrofolate (the active folate), 18 mg iron, 2,000 IU vitamin D3, 220 mcg iodine, and 100 mg choline. It suits most healthy women as a once‑daily preconception multi. If your Vitamin D, 25-Hydroxy or Ferritin are low, you may need extra targeted doses alongside it. Vegans and those with limited dairy or seafood also benefit from the included B12, iodine, and choline.
L‑5‑methyltetrahydrofolate is the folate form your cells use directly, which helps bypass common MTHFR gene variants and supports early fetal neural tube closure. Iodine fuels thyroid hormone production, and stable thyroid function (tracked with TSH, the pituitary signal that drives thyroid output) matters for ovulation and early pregnancy. Iron builds red blood cell mass ahead of rising needs, while vitamin D3 helps calcium absorption and immune balance. Choline supports fetal brain cell membrane growth, and B6 can ease early‑pregnancy nausea in some patients.
Take one tablet with food, ideally at a main meal to improve iron absorption and reduce nausea. Start at least 1 to 3 months before conception and continue through the first trimester; many keep a prenatal through breastfeeding. If you’re sensitive to iron, try evening dosing or a small snack. Separate coffee or tea by an hour, since tannins can reduce iron uptake. Add a separate DHA/EPA omega‑3 if your seafood intake is low.
Skip iron‑containing prenatals if you have hemochromatosis or very high Ferritin, and use a no‑iron option instead. If you take levothyroxine for thyroid disease, separate this by 4 hours because iron and calcium reduce absorption. Those with autoimmune thyroiditis should discuss the 220 mcg iodine with their clinician, as needs vary. Do not combine with other vitamin A supplements; this product uses beta‑carotene (a provitamin form), which is preferred in pregnancy.
Frequently asked questions
When should I start a prenatal if I’m trying to conceive?
Start 1 to 3 months before trying. Folate-dependent neural tube development happens very early, often before you miss a period. Starting early also lets you correct low Vitamin D, 25-Hydroxy or Ferritin alongside the prenatal.
Is methylfolate better than folic acid for pregnancy?
Methylfolate (L‑5‑MTHF) is the active form your cells use. It’s helpful if you carry common MTHFR variants or prefer to avoid folic acid. Clinically, either can work when taken consistently, but methylfolate removes a conversion step.
Does this have enough choline, or should I add more?
It provides 100 mg choline, a helpful base. Many diets fall short, and pregnancy needs are higher. If you rarely eat eggs or liver, consider an additional choline supplement or increase choline-rich foods.
Can I take this prenatal with DHA fish oil?
Yes. This doesn’t include DHA/EPA, so adding a separate omega‑3 is common, especially if you eat little seafood. DHA supports fetal brain and eye development. Check with your clinician if you have a bleeding disorder or take prescription anticoagulants.
What side effects should I expect from a prenatal?
Mild nausea or constipation from iron is most common. Taking it with food, hydrating, adding fiber, or using magnesium citrate at night can help. B6 in this formula may ease nausea for some. If symptoms persist, ask about switching iron forms.
How do caffeine or calcium affect iron in a prenatal?
Coffee, tea, and large calcium doses reduce iron absorption. Take the prenatal with water at a meal, and separate coffee, tea, or calcium-rich foods/supplements by about an hour.
Which labs are worth checking before pregnancy?
Vitamin D, 25-Hydroxy, Ferritin, and TSH are practical. If Vitamin D or iron stores are low, add targeted supplements temporarily, then retest in 8 to 12 weeks.
Is the vitamin A form safe during pregnancy?
Yes. It uses beta‑carotene, a provitamin A your body converts as needed. It avoids preformed retinol, which is the form linked to toxicity at high intakes.
How to take it & ingredients
Suggested use: Take one tablet per day, with food.
Active ingredients
1 tablet per serving · 90 servings
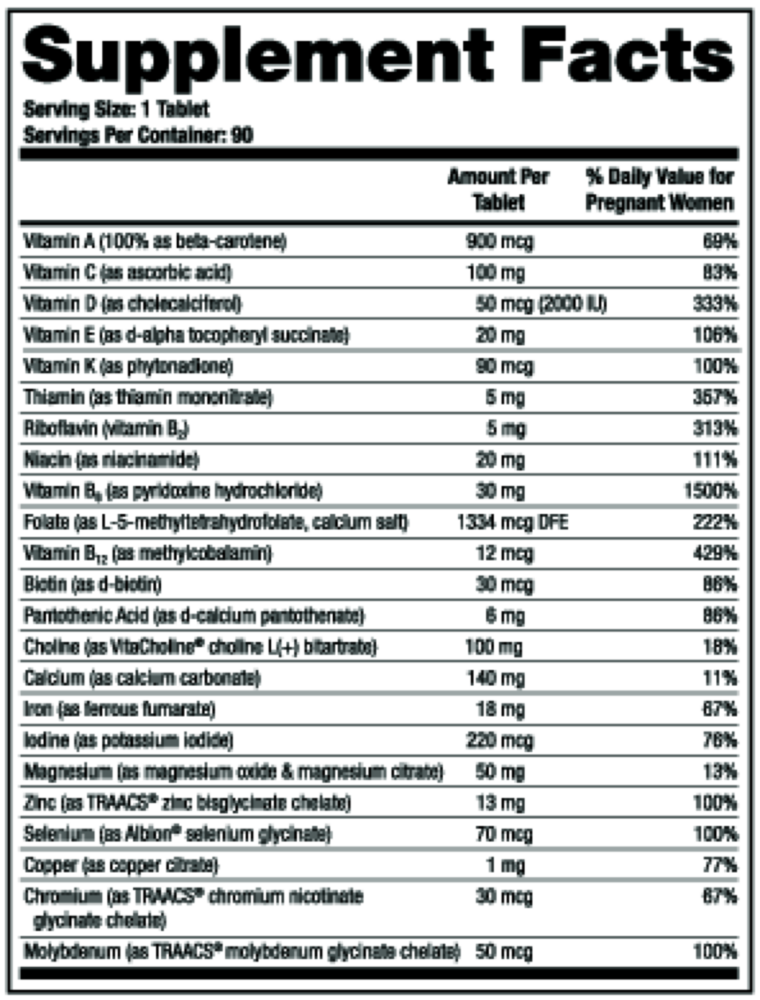
Vitamin A
100% as beta-carotene
100% as beta-carotene
900 mcg
Vitamin C
As ascorbic acid
As ascorbic acid
100 mg
Vitamin D
As cholecalciferol
As cholecalciferol
50 mcg
Vitamin E
As d-alpha tocopheryl succinate
As d-alpha tocopheryl succinate
20 mg
Vitamin K
As phytonadione
As phytonadione
90 mcg
Thiamin
As thiamin mononitrate
As thiamin mononitrate
5 mg
Riboflavin
Vitamin B2
Vitamin B2
5 mg
Niacin
As niacinamide
As niacinamide
20 mg
Vitamin B6
As pyridoxine hydrochloride
As pyridoxine hydrochloride
30 mg
Folate
As L-5-methyltetrahydrofolate, calcium salt
As L-5-methyltetrahydrofolate, calcium salt
1334 mcg DFE
Vitamin B12
As methylcobalamin
As methylcobalamin
12 mcg
Biotin
As d-biotin
As d-biotin
30 mcg
Pantothenic Acid
As d-calcium pantothenate
As d-calcium pantothenate
6 mg
Choline
As VitaCholine® choline L(+) bitartrate
As VitaCholine® choline L(+) bitartrate
100 mg
Calcium
As calcium carbonate
As calcium carbonate
140 mg
Iron
As ferrous fumarate
As ferrous fumarate
18 mg
Iodine
As potassium iodide
As potassium iodide
220 mcg
Magnesium
As magnesium oxide & magnesium citrate
As magnesium oxide & magnesium citrate
50 mg
Zinc
As TRAACS® zinc bisglycinate chelate
As TRAACS® zinc bisglycinate chelate
13 mg
Selenium
As Albion® selenium glycinate
As Albion® selenium glycinate
70 mcg
Copper
As copper citrate
As copper citrate
1 mg
Chromium
As TRAACS® chromium nicotinate glycinate chelate
As TRAACS® chromium nicotinate glycinate chelate
30 mcg
Molybdenum
As TRAACS® molybdenum glycinate chelate
As TRAACS® molybdenum glycinate chelate
50 mcg
Other ingredients: Microcrystalline cellulose, Croscarmellose sodium, Sodium nitrate, Vegetable stearic acid, Vegetable juice color, Silicon dioxide, Vegetable magnesium stearate, Hypromellose
Certifications
Benefits
Warnings
Customers also considered

Baby & Me 2
MegaFood
60 tablets
$47.99Save 21% with Subscribe & Save

Basic Prenatal
Thorne
90 capsules
$37.00Save 10% with Subscribe & Save

Essential for Women Postnatal Multivitamin - Citrus
Ritual
60 capsules
$44.99Save 20% with Subscribe & Save

Essential for Women Prenatal Multivitamin - Citrus
Ritual
60 capsules
$44.99Save 20% with Subscribe & Save