



Thorne
Betaine HCL & Pepsin by Thorne
225 capsules
Support Digestive Health and Nutrient Absorption$47.00
Purchase options
Practitioner-grade brand3rd-party testedFree shipping $50+
Gluten Free·Soy Free·Dairy Free·Milk Free
Thorne Betaine HCL & Pepsin overview
If you’re searching for betaine HCl because meals sit heavy, you bloat after protein, or you burp undigested food, you’re the use case. It’s also reasonable if Vitamin B12 or Ferritin (iron storage) run low despite eating well, since low stomach acid impairs absorption. Plant-forward eaters, adults over 40, and long-term users of acid suppressors in the past often land here. If you currently have frequent reflux burning, this is usually the wrong tool.
Stomach acid is the ignition for digestion. Betaine HCl increases stomach acidity, which converts pepsinogen into pepsin (the enzyme that breaks protein into smaller pieces). The lower pH also helps minerals like iron, calcium, magnesium, and zinc dissolve so they can be absorbed, and it curbs bacterial overgrowth higher up in the gut. Adequate acidity signals the small intestine to release bile and pancreatic enzymes, so downstream digestion runs on time.
Take 1 capsule with the first bites of a protein-containing meal; increase to 2 if one doesn’t change post-meal heaviness within a few days. Mid-meal timing works best, and avoid taking it without food. Most people feel lighter digestion within the first week; nutrient markers like Vitamin B12 or Ferritin shift over months. If you feel warmth, burning, or reflux, reduce the dose or stop.
Skip this if you have a history of stomach or duodenal ulcers, active gastritis, chronic reflux with esophageal damage, Barrett’s esophagus, or an untreated H. pylori infection. Avoid during pregnancy and breastfeeding, and in children. The pepsin is porcine, so it’s not suitable for vegetarians, vegans, or those avoiding pork for religious or allergy reasons. Post–bariatric surgery: use only with clinician guidance.
Don’t pair betaine HCl with acid-suppressing drugs like proton pump inhibitors (omeprazole, esomeprazole) or H2 blockers (famotidine), or with antacids; they directly oppose its effect. Use caution if you take daily NSAIDs (ibuprofen, naproxen), aspirin, corticosteroids, or bisphosphonates, which raise ulcer risk. If your hs-CRP (an inflammation marker) is elevated from reflux irritation, address that first. Thorne’s quality standards apply here; dose still needs clinical sense.
How do you know if low acid is the issue? The Heidelberg gastric pH test is the gold standard; routine labs don’t measure stomach acid directly. Will this fix reflux? If reflux is from true over-acid, no. If it’s from slow, poorly acidified emptying, careful low dosing can help, but stop if burning worsens. Can it replace digestive enzymes? It complements them; pepsin handles protein, while separate enzyme blends address carbs and fats.
Frequently asked questions
What is betaine HCl used for?
Primarily to increase stomach acidity for better protein breakdown and mineral absorption. People use it for heavy, lingering meals and for low Vitamin B12 or Ferritin despite adequate intake. It’s not a fix for active acid reflux or ulcers.
How long does betaine HCl take to work?
Digestive comfort changes are often felt within the first few meals to one week. Nutrient markers like Vitamin B12 or Ferritin take weeks to months to improve because body stores change slowly.
Can I take betaine HCl with a PPI or famotidine?
No. Proton pump inhibitors (omeprazole, esomeprazole) and H2 blockers (famotidine) reduce stomach acid and counteract betaine HCl. Combining them is contradictory and can confuse symptom tracking.
Should I take betaine HCl without food?
Don’t take it on an empty stomach. Always take it with the first bites of a meal that contains protein. Taking it without food increases the chance of warmth, burning, or nausea.
Does betaine HCl help with B12 and iron absorption?
It can. Adequate stomach acid is required to release Vitamin B12 from food proteins and to keep iron soluble. If your Vitamin B12 or Ferritin are low from poor absorption, improving acidity can help over time.
What are common side effects of betaine HCl?
The most common are warmth, burning, or reflux if the dose is too high or taken without food. Nausea can occur. Reduce the dose or stop if symptoms appear, and avoid entirely if you have a history of ulcers.
Is pepsin in this product vegetarian?
No. The pepsin here is porcine (from pork). It isn’t suitable for vegetarians, vegans, or those avoiding pork for religious or allergy reasons.
How do I test for low stomach acid?
The Heidelberg gastric pH test directly measures stomach acidity. Indirect clues include low Vitamin B12, high methylmalonic acid, or low Ferritin, but they aren’t specific. The baking soda test isn’t reliable.
How to take it & ingredients
Suggested use: Take 1-2 capsules with each meal or as recommended by your health professional.
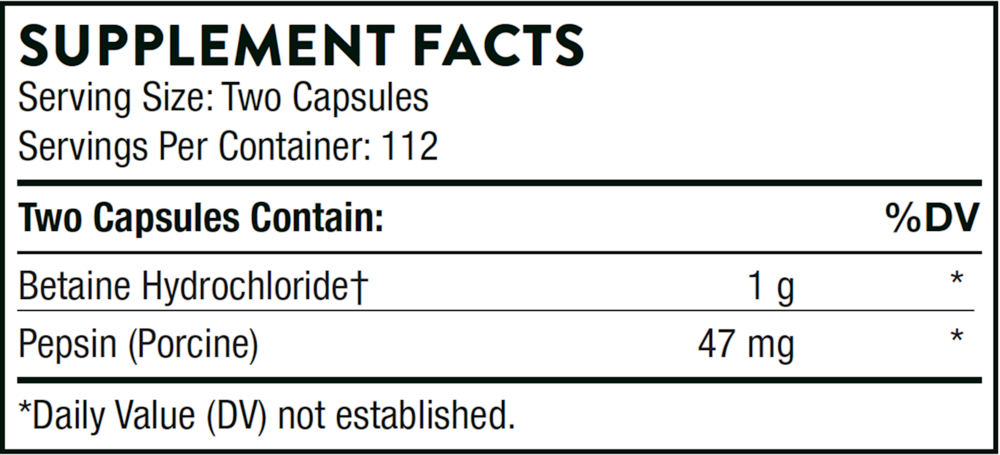
Active ingredients
2 capsules per serving
Betaine Hydrochloride (HCl)
1000 mg
Pepsin
Porcine
Porcine
47 mg
Other ingredients: Calcium Laurate, Hypromellose Capsule, Leucine, Silicon Dioxide
Certifications
Benefits
Warnings
