

Vitanica
Black Cohosh by Vitanica
60 capsules · 60-day supply
Standardized Extract Plus Whole Root$17.99
Purchase options
Practitioner-grade brand3rd-party testedFree shipping $50+
Vegan·Vegetarian·Gluten Free·Dairy Free·Egg Free·Fish Free·
Vitanica Black Cohosh overview
This formula provides a traditional botanical option in a daily capsule. It is a popular Native American and traditionally used women's herb, and it does not contain any phytoestrogens itself, so it suits adults who prefer a non-phytoestrogen botanical approach in their daily routine.
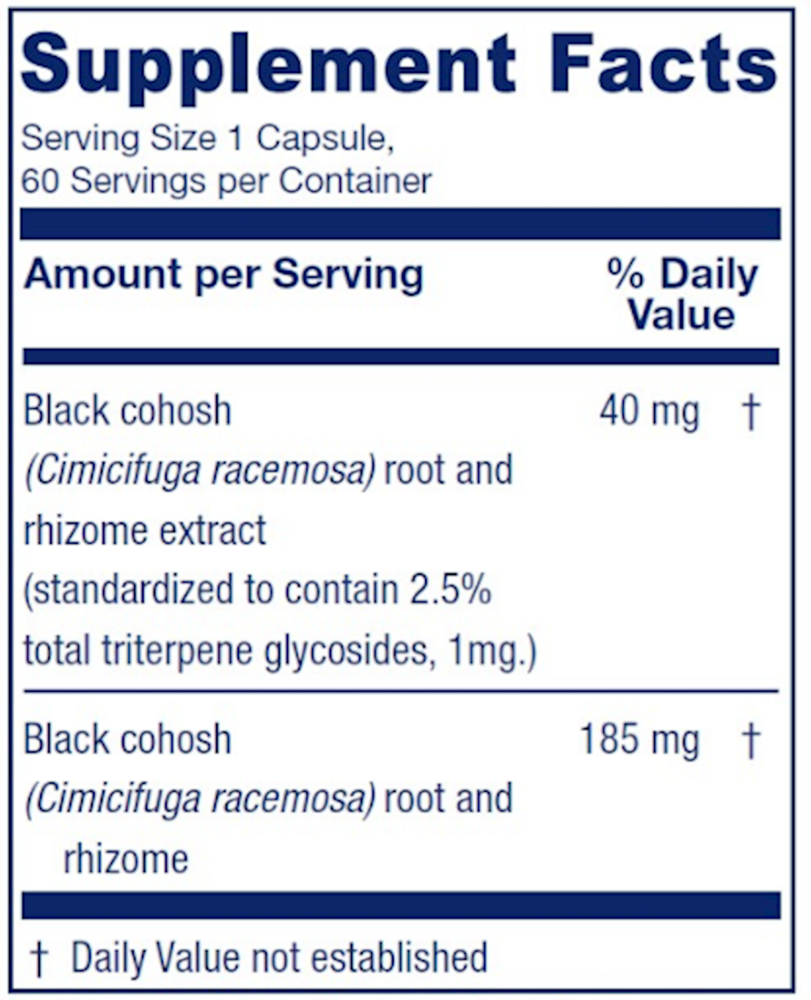
Each vegetarian capsule combines two complementary forms of black cohosh (Cimicifuga racemosa) root and rhizome. The 40 mg standardized extract is calibrated to 2.5% total triterpene glycosides (1 mg of triterpene glycosides per capsule), the well researched marker compounds in the herb. The 185 mg of dried root and rhizome powder represents the traditional whole-herb preparation. Together they provide both the studied standardized extract and the traditional botanical form in a single capsule.
Take one capsule once or twice daily, with or without food. Botanical support of this kind typically builds gradually, so allow several weeks of consistent daily use before assessing how it fits into your routine. If you find a single capsule daily is enough, that is also reasonable as long-term use.
If you take prescription medications, are pregnant or breastfeeding, or have a history of liver concerns, talk to your clinician before starting and review the warnings below.
Frequently asked questions
What is the difference between the standardized extract and the root powder in this capsule?
The 40 mg standardized extract is calibrated to a consistent 2.5% triterpene glycoside content (1 mg of triterpene glycosides per capsule), giving you a measured amount of the well researched marker compounds. The 185 mg of dried root and rhizome powder is the traditional whole-herb form used historically. Both are included in every capsule.
Does black cohosh contain phytoestrogens?
No. Black cohosh itself does not contain phytoestrogens, which is why it suits women who prefer a non-phytoestrogen botanical option in their daily routine.
How long should I take it before I notice anything?
Botanical support typically builds gradually. Many women allow several weeks of consistent daily use before assessing how the routine fits them. If you do not notice any change after a reasonable trial, it is reasonable to reassess with your clinician.
Can I take this with other supplements?
Black cohosh is generally taken as a stand-alone botanical in this formula, with one capsule once or twice daily. If you take other botanicals or supplements that influence the same pathways, review the combined routine with your clinician.
Is this product vegetarian?
Yes. The capsule shell is hydroxypropyl methylcellulose (a plant-derived vegetarian capsule). The only other inactive ingredient is calcium laurate. There are no animal-derived components.
What if I have a history of liver concerns?
Talk to your clinician before starting. Use caution with pre-existing liver conditions or if you take medications that affect liver enzymes, and stop use and contact your clinician if you notice dark urine, yellowing of the skin or eyes, or right-sided upper abdominal pain.
How should I store the bottle?
Store in a cool, dry place away from direct sunlight, and keep the bottle tightly closed between uses.
How to take it & ingredients
Suggested use: One capsule, once or twice daily; with or without food.
Active ingredients
1 capsule per serving · 60 servings
Black Cohosh
Cimicifuga racemosa, root and rhizome
Cimicifuga racemosa, root and rhizome
185 mg
Black Cohosh
Cimicifuga racemosa, root and rhizome, standardized to contain 2.5% total triterpene glycosides, 1mg
Cimicifuga racemosa, root and rhizome, standardized to contain 2.5% total triterpene glycosides, 1mg
40 mg
Other ingredients: Vegan capsule (hydroxypropyl methylcellulose, water), calcium laurate
Certifications
Benefits
Warnings
Customers also considered
Balance
Ortho Molecular Products
60 capsules
$47.90Save 10% with Subscribe & Save

Black Cohosh 2.5
Pure Encapsulations
120 capsules
$53.00Save 21% with Subscribe & Save

BreastBlend™
Vitanica
90 capsules
$51.99Save 19% with Subscribe & Save

CDG EstroDIM
Ortho Molecular Products
60 capsules
$103.73Save 10% with Subscribe & Save