


Allergy Research Group
Selenium Solution 100 mcg by Allergy Research Group
236 milliliters · 94-day supply
Essential Selenium for Antioxidant Support and Immune Function$16.99
Purchase options
Practitioner-grade brand3rd-party testedFree shipping $50+
Gluten Free·Soy Free·Dairy Free·Egg Free·Milk Free·Tree Nut Free·
Allergy Research Group Selenium Solution overview
If your Selenium, Serum is low or you eat a very low‑selenium diet (little seafood, eggs, or Brazil nuts), liquid selenium helps you replete gently. It’s also practical if you prefer drops to pills, have trouble swallowing, or need precise, smaller increments. People with autoimmune thyroiditis and high Thyroid Peroxidase Antibodies (TPO Ab, the marker of thyroid autoimmunity) sometimes use selenium under clinician guidance, especially when status is low.
Selenium is required to build selenoproteins like glutathione peroxidase (an enzyme that clears peroxides to protect cells), thioredoxin reductase (a redox regulator), and deiodinases (the enzymes that convert T4 to the active thyroid hormone T3). Sodium selenite is an inorganic form that the body converts directly into these proteins without being stored nonspecifically in tissues, which is one reason clinicians pick it for targeted repletion.
Each 1/2 teaspoon provides 100 mcg. The label suggests three servings daily, but many adults land in the 100–200 mcg per day range for maintenance; use higher intakes only if your level is low and you’re being monitored. Take with or without food, any time of day. If you use high‑dose vitamin C (1,000 mg or more), separate by a few hours to avoid reducing selenite’s absorption.
If your Selenium, Serum is already high, skip extra selenium. Hair or nail brittleness, a metallic taste, or gastrointestinal upset can signal excess. Pregnant or breastfeeding adults should stay closer to maintenance dosing unless a clinician is following labs. Those on dialysis or with significant kidney disease need individualized dosing. Selenium is not for cancer prevention; large trials didn’t show benefit.
Recheck Selenium, Serum after 8 to 12 weeks to confirm you’re in range without creeping into excess. If you’re taking it for thyroid reasons, track TSH (the pituitary signal to the thyroid), Free T4, and TPO Ab alongside symptoms. Expect antioxidant enzyme activity to improve within 4 to 8 weeks once intake is adequate.
Frequently asked questions
How much selenium should I take daily?
For maintenance, many adults use 100–200 mcg per day from supplements, adjusting for diet. Higher intakes are for documented low levels and short-term repletion under clinician guidance. Avoid chronically exceeding common upper limits to prevent hair/nail changes and stomach upset.
How long does selenium take to help thyroid health?
If you were low, expect 8–12 weeks to see changes on labs. Antibody shifts (TPO Ab) in autoimmune thyroiditis are modest and inconsistent across studies. Track TSH and Free T4 with your clinician rather than relying on symptoms alone.
Can I take selenium with levothyroxine?
Yes, there’s no direct absorption clash. Take levothyroxine on an empty stomach as usual, and take selenium at another time of day. Monitor TSH and Free T4 as selenium status changes can subtly affect thyroid hormone conversion.
Does vitamin C interfere with selenium?
High-dose vitamin C can chemically reduce selenite and may lower its absorption. If you take 1,000 mg or more of vitamin C, separate dosing by a few hours. This is less of a concern with small vitamin C doses in food or multivitamins.
What are signs of too much selenium?
Early signs include a metallic taste, nausea, diarrhea, brittle hair or nails, and a garlic-like breath odor. Stop supplementing and check Selenium, Serum if these occur. Very high intakes can be toxic, so don’t exceed labeled directions without supervision.
Is sodium selenite better than selenomethionine?
They’re different tools. Selenomethionine is well absorbed and stored broadly in proteins, which can raise blood levels more. Sodium selenite is used for targeted repletion of selenoproteins without as much nonspecific tissue storage. Clinicians choose based on goals and labs.
Can selenium help with mercury detox?
Selenium can bind mercury and supports antioxidant enzymes, but it isn’t a chelator. Don’t use it as a stand-alone detox strategy. If mercury exposure is a concern, work with a clinician and focus on reducing sources and appropriate testing.
Does selenium prevent colds or cancer?
It doesn’t reliably prevent infections or cancer. Large trials, including the SELECT trial, found no cancer-prevention benefit in well-nourished adults. Use selenium to correct low levels and sustain selenoprotein function, not as a disease shield.
How to take it & ingredients
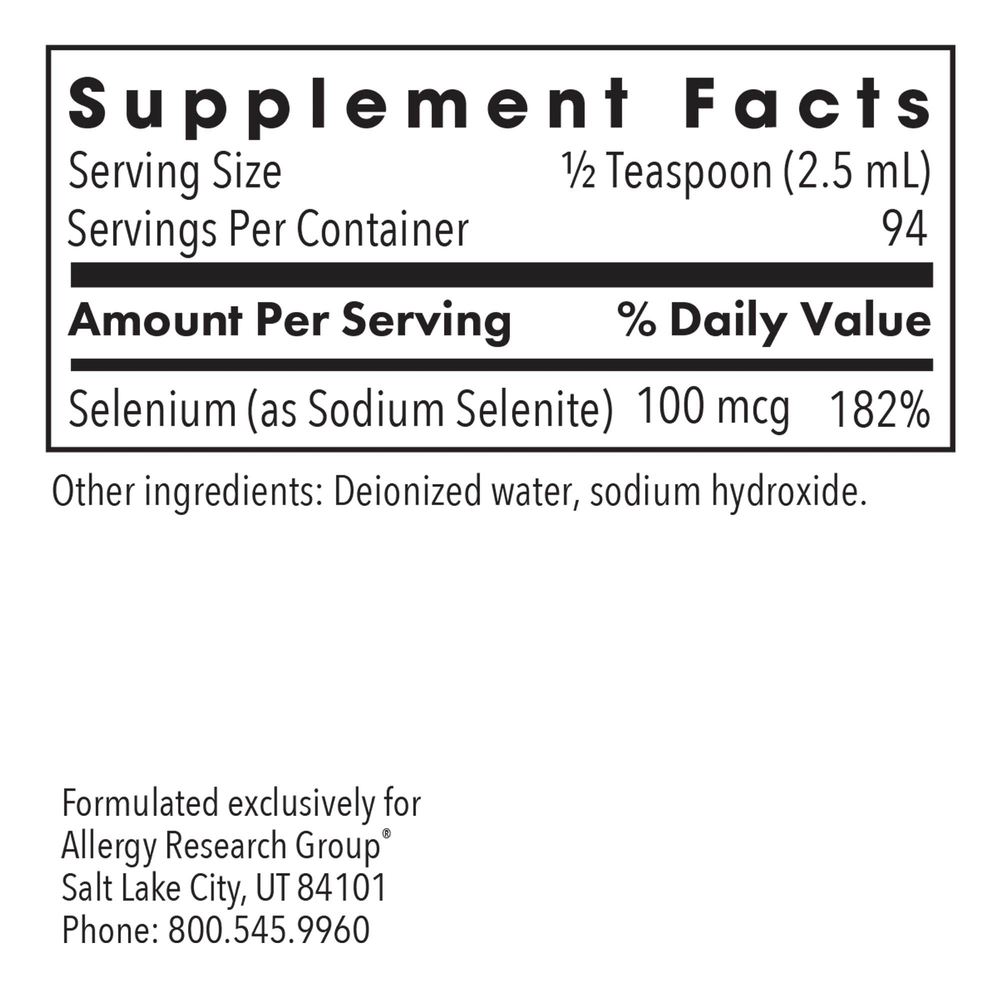
Suggested use: As a dietary supplement, take 1/2 teaspoon three times daily, or as directed by a healthcare practitioner. Do not exceed daily dose.
Active ingredients
1/2 teaspoon (2.5 ml) per serving · 94 servings
Selenium
As Sodium Selenite
As Sodium Selenite
100 mcg
Other ingredients: Deionized water, Sodium hydroxide
Certifications
Benefits
Warnings
Customers also considered
Ortho Molecular Products
Reacted Selenium
90 capsules
$37.80extra 10% off with Subscribe & Save

Thorne
Selenium
60 capsules
$14.00extra 10% off with Subscribe & Save

Pure Encapsulations
Selenium
60 capsules
$14.50extra 17% off with Subscribe & Save

Nature’s Way
Selenium 200 mcg
100 capsules
$11.99extra 17% off with Subscribe & Save