


Biotics Research
Red Yeast Rice 2400 mg by Biotics Research
90 capsules · 30-day supply
Supports Healthy Cholesterol Levels with Natural Red Yeast Rice$25.99
This item is currently out of stockGet notified when this item is back in stock
Practitioner-grade brand3rd-party testedFree shipping $50+
Gluten Free·Dairy Free·Milk Free
Biotics Research Red Yeast Rice overview
If you’re searching for red yeast rice for high cholesterol, this fits adults with mildly to moderately elevated LDL cholesterol who prefer a non-prescription route or who can’t tolerate statins. It’s most appropriate if your Lipid Panel shows high LDL-C or non-HDL-C, or your ApoB (the number of atherogenic particles) is above your target. If you already have cardiovascular disease or very high risk, prescription therapy remains first-line — use red yeast rice only under clinician guidance.
Red yeast rice naturally contains monacolin K, which is chemically the same as lovastatin. It inhibits HMG‑CoA reductase, the liver enzyme that makes cholesterol, so LDL drops about 15–25% in most responders within 4 to 8 weeks. Triglycerides often fall modestly, while hs-CRP (a blood marker of inflammation) changes are small and not the main reason to take it. Reality check: monacolin content varies by brand, and the FDA treats high-monacolin products as drugs, so effects can differ between bottles.
The suggested 2,400 mg per day (three capsules) is the common clinical amount, best taken with your evening meal to improve tolerance. Avoid grapefruit, which can raise monacolin levels. Recheck your Lipid Panel or ApoB after 8–12 weeks, then every 3–6 months. If you develop unexplained muscle aches, stop and talk to your clinician, who may check CK (creatine kinase, a muscle injury marker). Many clinicians pair red yeast rice with CoQ10 100–200 mg to offset statin-like depletion.
Treat red yeast rice like a low-dose statin. Do not combine with a prescription statin or with gemfibrozil. Skip during pregnancy or breastfeeding, with active liver disease, heavy alcohol use, or untreated hypothyroidism (which increases muscle risk). Avoid interacting drugs like clarithromycin or erythromycin, azole antifungals, HIV protease inhibitors, cyclosporine, and large amounts of niacin. Choose products tested for citrinin, a mold toxin that can form during fermentation.
Frequently asked questions
Does red yeast rice really lower LDL cholesterol?
Yes. Because it contains monacolin K (lovastatin), most responders see LDL drop about 15–25%. The effect depends on the monacolin content, which varies by brand, and your baseline diet and genetics.
How long does red yeast rice take to work?
Plan on 4–8 weeks for a meaningful change. Recheck your Lipid Panel or ApoB at 8–12 weeks to confirm response, then adjust dose or strategy with your clinician.
Is red yeast rice the same as a statin?
Functionally, yes. Its active, monacolin K, is chemically identical to lovastatin and shares benefits and risks. That means similar interactions, liver considerations, and rare muscle side effects.
What labs should I monitor on red yeast rice?
Track LDL-C, non-HDL-C, and ApoB to gauge benefit. Many clinicians also check liver enzymes (ALT, AST) at baseline and after 8–12 weeks, and CK if muscle symptoms occur.
Can I take red yeast rice with a statin?
No. Combining them duplicates therapy and raises risk for muscle injury and liver enzyme elevations. If you’re on a statin, discuss alternatives with your prescriber instead.
Should I take CoQ10 with red yeast rice?
It’s reasonable. Like statins, red yeast rice can lower your body’s CoQ10 levels. Many clinicians suggest 100–200 mg daily, especially if you notice muscle fatigue or cramps.
Is grapefruit a problem with red yeast rice?
Yes. Grapefruit can increase monacolin K levels and side-effect risk. Avoid grapefruit and its juice while taking red yeast rice.
Is red yeast rice safe during pregnancy or breastfeeding?
Avoid it. Because it acts like a statin, red yeast rice isn’t considered safe in pregnancy or while breastfeeding. Use diet and clinician-guided options instead.
How to take it & ingredients
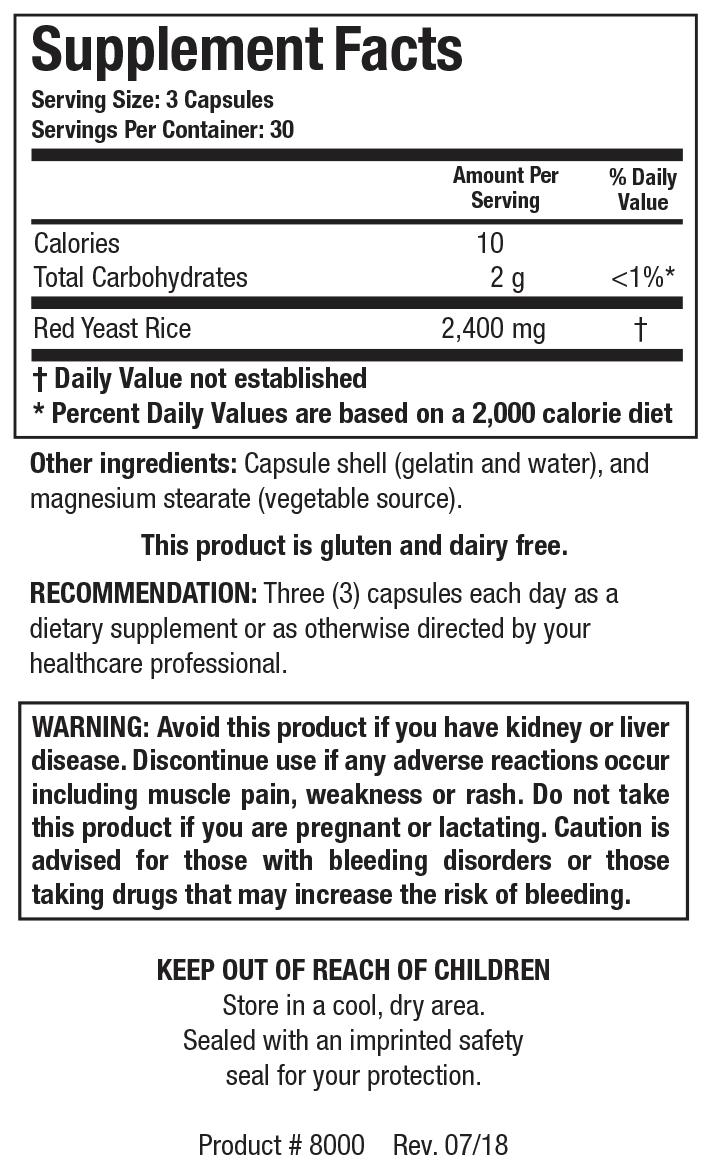
Suggested use: Take three capsules daily as a dietary supplement or as directed by your healthcare professional.
Active ingredients
3 capsules per serving · 30 servings
Red Yeast Rice
Monascus purpureus
Monascus purpureus
2400 mg
Other ingredients: Gelatin, Water, Magnesium stearate (vegetable source)
Certifications
Benefits
Warnings
