

New Chapter
Bone Strength Take Care by New Chapter
90 tablets · 30-day supply
Comprehensive Bone Support with Calcium, Vitamin D, and Magnesium$54.99
Purchase options
Practitioner-grade brand3rd-party testedFree shipping $50+
Vegetarian·Kosher·Gluten Free·Artificial Color Free·Artificial Flavor Free
New Chapter Bone Strength Take Care overview
If your DEXA scan shows low bone density or your Vitamin D, 25-Hydroxy is in the lower range, algae calcium is a practical way to fill a calcium gap without the constipation many get from calcium carbonate. It fits postmenopausal women, dairy-avoiders, vegans on restrictive diets, and long‑term acid-reducer users whose stomach acid is low. If your diet already supplies most of your calcium, use fewer tablets rather than overshooting.
This formula uses a red marine algae mineral matrix, not rock. The calcium comes packaged with magnesium and trace minerals, which many patients find gentler on the gut. Vitamin D3 (the form your skin makes) improves calcium absorption and helps rein in parathyroid hormone, the signal that pulls calcium from bone. Vitamin K1 and K2 MK‑7 activate osteocalcin (the protein that loads calcium into bone) and matrix Gla protein (which helps keep calcium out of arteries). The strontium here is a low trace amount; it won’t inflate DEXA the way high-dose strontium drugs can.
Take three tablets daily with food, ideally split into two or three meals, since the gut absorbs calcium better in doses of about 500 mg or less at a time. If you already get 700–800 mg from food, one or two tablets usually makes more sense than three. Expect changes in bone turnover markers like P1NP and CTX within 8–12 weeks; DEXA changes are assessed over 6–24 months.
Separate calcium by 4 hours from levothyroxine, certain antibiotics (tetracyclines, fluoroquinolones), and minerals like iron or zinc because it blocks absorption. Vitamin K in this formula conflicts with warfarin; do not use together unless your prescriber adjusts dosing. Thiazide diuretics can raise blood calcium, so monitor with your clinician. If you have a history of high calcium, recurrent kidney stones, hyperparathyroidism, sarcoidosis, or advanced kidney disease, skip calcium supplements and get individualized care.
Frequently asked questions
Is algae calcium better absorbed than calcium carbonate?
Absorption is similar on paper, but many people tolerate algae calcium better with fewer constipation complaints. Taken with meals in split doses, both absorb well; the advantage here is gentler digestion and bundled cofactors like vitamin D3 and K2.
How long until I see results on bone density?
Bone density changes are slow. Plan on 6–24 months between DEXA scans. You can see earlier shifts in bone turnover labs (P1NP, CTX) within 8–12 weeks when intake and vitamin D status improve.
Can I take this calcium with thyroid medication?
Not at the same time. Calcium binds levothyroxine and blocks its absorption. Take thyroid medication on an empty stomach, and wait at least 4 hours before taking calcium.
Does this calcium cause constipation or gas?
It’s typically easier on the gut than calcium carbonate. Taking split doses with meals and staying hydrated reduces constipation risk. If you still get constipated, lower the dose or adjust fiber and magnesium from food.
Is vitamin K2 safe with blood thinners?
Not with warfarin. Vitamin K (including K2 MK‑7) interferes with warfarin’s action. Direct oral anticoagulants like apixaban or rivaroxaban aren’t vitamin K–dependent, but discuss any supplement change with your prescriber.
Does calcium increase heart disease risk?
When calcium is taken with adequate vitamin D and K, cardiovascular concerns appear low in most data. Vitamin K helps activate proteins that keep calcium out of arteries. Still, avoid megadoses and match your supplement to your actual dietary gap.
Can men use this calcium supplement?
Yes. Men with low dietary calcium, low Vitamin D, 25-Hydroxy, or low bone density on DEXA can benefit. The same dosing, separation from medications, and monitoring guidance apply.
Is this safe if I’ve had kidney stones?
Use caution. People with recurrent calcium oxalate stones should get personalized advice. Calcium from food is preferred; if a supplement is used, take it with meals and review your urine chemistry with a clinician.
How to take it & ingredients
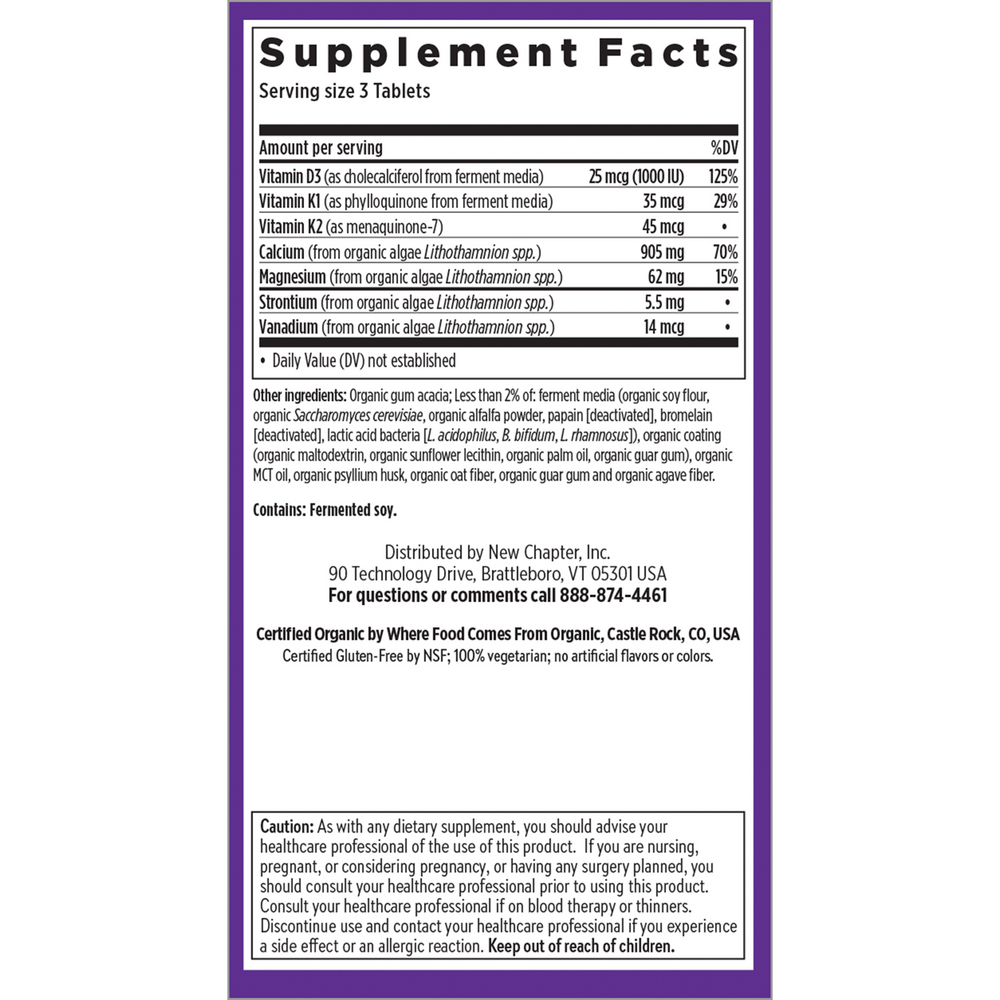
Suggested use: Take three tablets daily with food.
Active ingredients
3 tablets per serving · 30 servings
Vitamin D3
Cholecalciferol from ferment media
Cholecalciferol from ferment media
25 mcg, 1000 IU
Vitamin K1
Phylloquinone from ferment media
Phylloquinone from ferment media
35 mcg
Vitamin K2
Menaquinone-7
Menaquinone-7
45 mcg
Organic Algae Lithothamnion
Lithothamnion calcareum and Lithothamnion corallioides
Lithothamnion calcareum and Lithothamnion corallioides
974.51 mg
Calcium
From organic algae Lithothamnion
From organic algae Lithothamnion
905 mg
Magnesium
From organic algae Lithothamnion
From organic algae Lithothamnion
62 mg
Strontium
From organic algae Lithothamnion
From organic algae Lithothamnion
5.5 mg
Silica
From organic algae Lithothamnion
From organic algae Lithothamnion
2 mg
Vanadium
From organic algae Lithothamnion
From organic algae Lithothamnion
14 mcg
Other ingredients: Organic barley grass powder, Organic gum acacia, Ferment media (organic soy flour, organic Saccharomyces cerevisiae, organic alfalfa powder, papain (deactivated), bromelain (deactivated), Lactobacillus acidophilus, Bifidobacterium bifidum, Lactobacillus rhamnosus), Organic coating (organic maltodextrin, organic sunflower lecithin, organic palm oil, organic guar gum), Silica
Certifications
Benefits
Warnings
Customers also considered

AlgaeCal Inc.
AlgaeCal Plus
120 capsules
$81.99extra 20% off with Subscribe & Save

Pure Encapsulations
Magnesium Citrate
180 capsules
$34.50extra 19% off with Subscribe & Save

Ortho Molecular Products
OsteoBase
90 capsules
$39.68extra 10% off with Subscribe & Save

Ortho Molecular Products
OsteoPrev®
120 capsules
$86.19extra 10% off with Subscribe & Save