

Ortho Molecular Products
OsteoPrev® by Ortho Molecular Products
120 capsules · 30-day supply
Comprehensive Bone Support with Essential Vitamins and Minerals$86.19
Purchase options
Practitioner-grade brand3rd-party testedFree shipping $50+
Gluten Free·Yeast Free·Artificial Color Free·Artificial Flavor Free
Ortho Molecular Products OsteoPrev® overview
If your DEXA scan shows declining bone density or your Vitamin D, 25-Hydroxy is low, this bone density supplement is a practical next step. It fits post‑menopausal women, smaller-framed adults, people on low-calcium diets, and anyone limiting dairy. It also suits long-term proton pump inhibitor users and those on aromatase inhibitors, where bone loss risk is higher. If you already take high-dose calcium, this formula layers in vitamin K2 and ipriflavone without overloading calcium.
Ipriflavone (600 mg/day) slows osteoclasts, the cells that break down bone, and in trials preserved bone density when paired with calcium. Vitamin K2 as MK‑7 activates osteocalcin (the protein that locks calcium into bone) and matrix Gla protein (the protein that helps keep calcium out of arteries). Vitamin D3 1,000 IU improves calcium absorption and tamps down parathyroid hormone, the signal that pulls calcium from bone. Boron, magnesium, and trace minerals round out bone remodeling support.
Take four capsules daily in two divided doses with meals, which improves calcium and magnesium uptake. The calcium here (250 mg/day) is a modest maintenance amount; if your dietary calcium is low, add food sources or a separate calcium to reach your target. Expect changes in bone turnover markers like CTX and P1NP within 8–12 weeks, with DEXA changes judged over 6–12 months. Recheck Vitamin D, 25-Hydroxy after 8–12 weeks and adjust D3 if still low.
Skip this if you take warfarin (Coumadin); the high vitamin K1 and K2 will interfere with dosing. Separate by at least four hours from thyroid hormone, tetracycline or quinolone antibiotics. Avoid in pregnancy and breastfeeding, as ipriflavone data are limited. If you have high blood calcium, recurrent calcium kidney stones, or conditions that raise calcium like sarcoidosis, use only with clinician guidance and monitor serum calcium and PTH.
Frequently asked questions
What does ipriflavone do for bone density?
Ipriflavone reduces bone breakdown by dialing down osteoclast activity. In studies, 600 mg/day with calcium helped preserve bone density in post‑menopausal women. It’s an add-on to adequate calcium, vitamin D3, and vitamin K2, not a stand‑alone fix.
How long until I see results on a DEXA scan?
Bone density shifts slowly. Plan on 6–12 months before a DEXA scan shows a measurable change. Earlier signals happen faster: bone turnover markers (CTX, P1NP) often move within 8–12 weeks, and Vitamin D, 25-Hydroxy responds over that same window.
Is the calcium dose enough on its own?
It’s a maintenance dose. Most adults need additional calcium from food to meet daily needs. If your diet is light on dairy or calcium-rich plants, pair this formula with a separate calcium to reach your target under clinician guidance.
Can I take this with bisphosphonates or denosumab?
Often yes, but coordinate timing. Calcium and magnesium can interfere with absorption of some oral drugs, so take them at a different time of day. Your clinician may use this alongside prescription therapy to improve nutrient status and turnover markers.
Does vitamin K2 interfere with blood thinners?
Yes for warfarin (Coumadin). Vitamin K1 and K2 affect warfarin dosing and stability, so avoid this product on warfarin unless your prescriber specifically manages it. Direct oral anticoagulants are not vitamin K–dependent, but confirm with your doctor.
Any side effects from ipriflavone or minerals?
Most tolerate it well. Possible effects include mild GI upset or headache. Rarely, ipriflavone has been linked to low white blood cell counts; stop and contact your clinician if you develop unexplained infections or fevers.
Can men use this bone density supplement?
Yes. While much research involves post‑menopausal women, the mechanisms—adequate D3, K2 activation of osteocalcin, and mineral repletion—apply to men with low dietary calcium or other bone risk factors. Monitor with DEXA and lab markers.
What labs should I monitor while taking it?
Track Vitamin D, 25-Hydroxy, serum calcium, and parathyroid hormone. For dynamics, follow bone turnover markers like CTX and P1NP at baseline and 8–12 weeks. Use DEXA every 1–2 years to assess bone density changes.
How to take it & ingredients
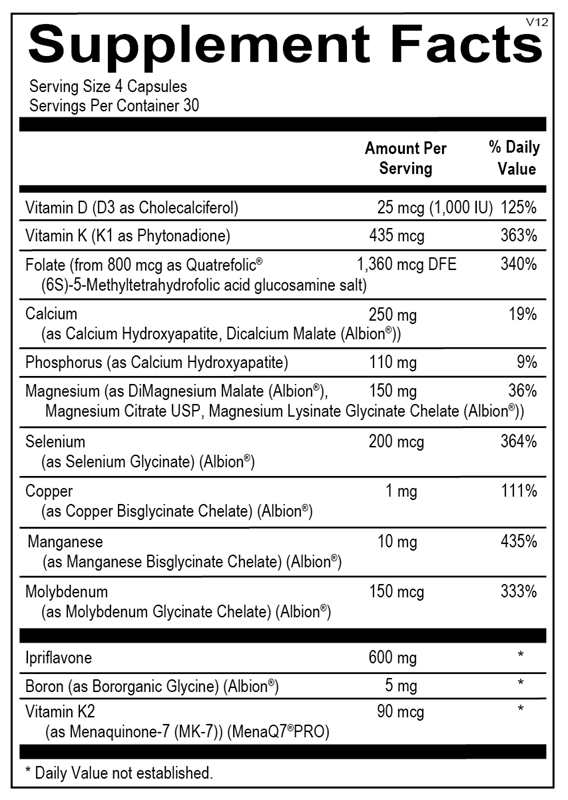
Suggested use: 4 capsules per day in divided doses or as recommended by your health care professional.
Active ingredients
4 capsules per serving · 30 servings
Vitamin D
D3 as Cholecalciferol
D3 as Cholecalciferol
25 mcg, 1000 IU
Vitamin K
K1 as Phytonadione
K1 as Phytonadione
435 mcg
Folate
From 800 mcg as Quatrefolic® (6S)-5-Methyltetrahydrofolic acid glucosamine salt
From 800 mcg as Quatrefolic® (6S)-5-Methyltetrahydrofolic acid glucosamine salt
1360 mcg DFE
Calcium
As Calcium Hydroxyapatite, Dicalcium Malate (Albion®)
As Calcium Hydroxyapatite, Dicalcium Malate (Albion®)
250 mg
Phosphorus
As Calcium Hydroxyapatite
As Calcium Hydroxyapatite
110 mg
Magnesium
As DiMagnesium Malate (Albion®), Magnesium Citrate USP, Magnesium Lysinate Glycinate Chelate (Albion®)
As DiMagnesium Malate (Albion®), Magnesium Citrate USP, Magnesium Lysinate Glycinate Chelate (Albion®)
150 mg
Selenium
As Selenium Glycinate (Albion®)
As Selenium Glycinate (Albion®)
200 mcg
Copper
As Copper Bisglycinate Chelate (Albion®)
As Copper Bisglycinate Chelate (Albion®)
1 mg
Manganese
As Manganese Bisglycinate Chelate (Albion®)
As Manganese Bisglycinate Chelate (Albion®)
10 mg
Molybdenum
As Molybdenum Glycinate Chelate (Albion®)
As Molybdenum Glycinate Chelate (Albion®)
150 mcg
Ipriflavone
600 mg
Boron
As Bororganic Glycine (Albion®)
As Bororganic Glycine (Albion®)
5 mg
Vitamin K2
As Menaquinone-7 (MK-7) (MenaQ7®PRO)
As Menaquinone-7 (MK-7) (MenaQ7®PRO)
90 mcg
Other ingredients: Hypromellose (Natural Vegetable Capsules), Microcrystalline Cellulose, Magnesium Stearate, Silicon Dioxide
Certifications
Benefits
Warnings
Customers also considered

AlgaeCal Inc.
AlgaeCal Plus
120 capsules
$81.99extra 20% off with Subscribe & Save
New Chapter
Bone Strength Take Care
60 tablets
$40.99extra 20% off with Subscribe & Save

Pure Encapsulations
Magnesium Citrate
180 capsules
$34.50extra 19% off with Subscribe & Save

Ortho Molecular Products
OsteoBase
90 capsules
$39.68extra 10% off with Subscribe & Save