

Ortho Molecular Products
BioPC Pro by Ortho Molecular Products
321 grams
Essential Phospholipids for Cellular Health and Membrane Support$72.09
Purchase options
Practitioner-grade brand3rd-party testedFree shipping $50+
Gluten Free·Corn Free·Yeast Free·Artificial Color Free·Artificial Flavor Free
Ortho Molecular Products BioPC Pro overview
If you’re watching ALT on your liver panel and your triglycerides run high, a phosphatidylcholine supplement can fit into a plan to reduce liver fat patterns. It’s also useful if your diet is low in choline-rich foods (few eggs or organ meats), if fat digestion feels heavy after meals, or if focus dips during very low‑fat dieting. People with low or borderline choline intake, modestly elevated hs-CRP (an inflammation marker), or brain fog often notice steadier energy and digestion.
Phosphatidylcholine, phosphatidylinositol, phosphatidylethanolamine, and phosphatidic acid are the core phospholipids that make up your cell and mitochondrial membranes. Replenishing them improves membrane fluidity and repair, which helps receptors and enzymes signal cleanly. In the liver, phosphatidylcholine helps package fat into VLDL particles (the form your liver uses to export triglycerides), easing fat buildup and often nudging ALT down within 8–12 weeks. As a choline source, it also feeds acetylcholine (a focus and memory neurotransmitter) and supports homocysteine recycling.
Take one scoop daily with a meal for better absorption, mixed in juice or a shake, or sprinkled on food. If you’re sensitive, split the scoop into two meals for a week, then consolidate. Pairing with omega-3 fish oil or an Omega-3 Index–guided seafood plan is common in lipid clinics. Recheck relevant labs (ALT, AST, triglycerides, homocysteine) after 8–12 weeks to judge response.
If you develop a fishy body odor or burps, that’s trimethylamine buildup from choline metabolism; lowering the dose or using a probiotic approach can help. Check the label for soy sourcing if you have a soy allergy. Very high choline intakes can worsen depressive mood in a small minority; if mood shifts, stop and discuss. Pregnancy and breastfeeding often need more choline than diet provides, but set the dose with your clinician.
Frequently asked questions
What is phosphatidylcholine used for?
Primarily for liver fat handling, bile flow, and membrane repair, with secondary benefits for focus and fat digestion. Clinicians track ALT, AST, triglycerides, and sometimes homocysteine to gauge response over 8–12 weeks.
How long does phosphatidylcholine take to work?
Digestive comfort can improve within 1–2 weeks. Lab changes like lower ALT or triglycerides, when they occur, are usually seen after 8–12 weeks of daily use alongside diet changes.
Can I take phosphatidylcholine with fish oil?
Yes. They’re complementary: phosphatidylcholine supports fat export from the liver, and fish oil (EPA/DHA) lowers liver fat production. Many lipid clinics pair them and recheck triglycerides in 8–12 weeks.
Does phosphatidylcholine raise TMAO?
Choline can raise TMAO (a gut-microbe metabolite) in some people. The clinical meaning is debated. If you’re concerned, prioritize seafood, fiber, and consider probiotics; discuss testing or alternatives with your clinician.
Is phosphatidylcholine safe long term?
Generally yes at typical supplemental doses. Common side effects are mild GI upset or a fishy odor. People with soy allergy should verify the source. Long-term use should be guided by periodic lab review.
Should I take phosphatidylcholine with food?
Yes. Taking it with a meal improves absorption and reduces stomach upset. Mixing the powder in a smoothie or juice is an easy way to take the full serving.
Who should avoid phosphatidylcholine?
Avoid if you have a known soy allergy and the product is soy-derived. If mood worsens or you notice persistent fishy odor, stop and reassess. In pregnancy or breastfeeding, set dosing with your clinician.
Will phosphatidylcholine lower my triglycerides?
It can help by improving liver fat export, especially when paired with diet and omega-3s. Some people see modest triglyceride drops in 8–12 weeks, but responses vary and should be tracked on a lipid panel.
How to take it & ingredients
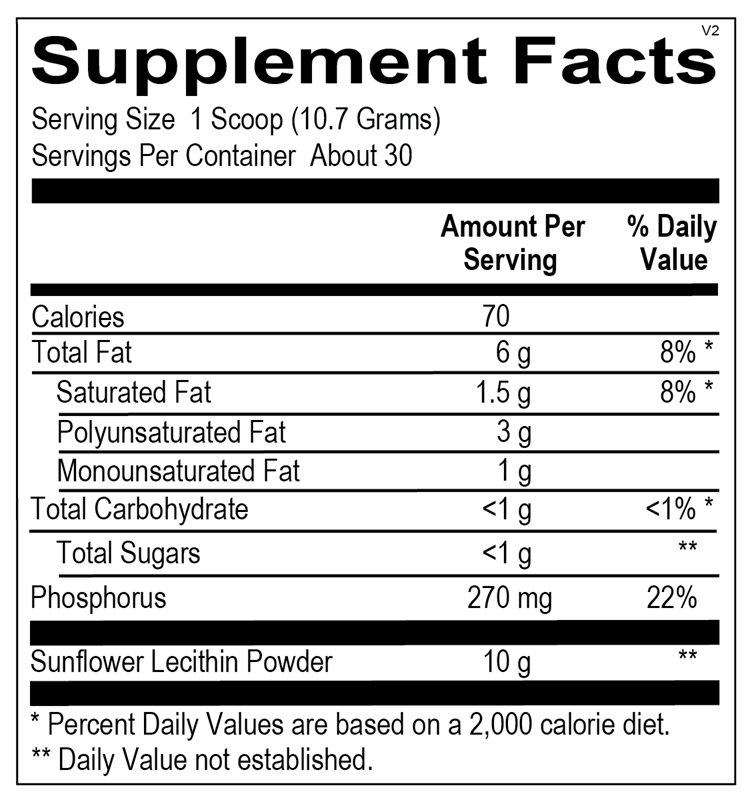
Suggested use: 1 scoop (10.7 grams) per day with a meal or as recommended by your health care professional. May be mixed in juice or shakes, or sprinkled on food.
Active ingredients
1 scoop (10.7 g) per serving
Phosphatidylcholine
2500 mg
Phosphatidylinositol
2000 mg
Phosphatidylethanolamine
1000 mg
Phosphatidic acid
400 mg
Other ingredients: Silicon Dioxide
Certifications
Benefits
Warnings
