

Ortho Molecular Products
Ortho Biotic 100 by Ortho Molecular Products
30 capsules · 30-day supply
Advanced Probiotic Blend for Digestive and Immune Health$XX.XX$91.41retail
Purchase option
10% below MSRP3rd-party tested for purity & potencyFree shipping $50+
Vegan·Vegetarian·Gluten Free·Soy Free·Corn Free·Yeast Free·
Ortho Molecular Products Ortho Biotic 100 overview
If you just finished antibiotics and want to reduce loose stools, a high dose probiotic is the practical choice. One capsule delivers 100 billion CFU, which suits short-term gut rebuilding after antibiotics, travel diarrhea, or a tough stomach bug. It also fits patients whose stool testing shows low Lactobacillus or Bifidobacterium, or low secretory IgA (the antibody that guards your gut lining). For mild, day-to-day upkeep, this potency is usually more than you need.
Multiple Lactobacillus and Bifidobacterium species compete with opportunists, make acids that lower gut pH, and produce short‑chain fatty acids like butyrate (fuel for colon cells). That combination improves stool form and reduces post‑infection gas for many people within 1 to 2 weeks. These bacteria also nudge immune balance in the gut, which is why some users see fewer antibiotic‑associated issues. Big claims about curing bloating or fixing the immune system don’t hold up consistently.
Take one capsule daily with a meal for better tolerance. During an antibiotic course, separate the probiotic by at least 2 to 3 hours, then continue daily for 2 to 4 weeks after the last antibiotic dose. Most people notice stool changes within 7 to 14 days; give it a full month for steadier patterns. This is a repletion-style dose. For long-term maintenance once you’re stable, many step down to a lower‑CFU probiotic.
Avoid probiotics if you have a central venous catheter, are severely immunocompromised (active chemotherapy, uncontrolled HIV, post‑transplant), or are critically ill—rare bloodstream infections have been reported in these settings. If you have small intestinal bacterial overgrowth, high doses can worsen bloating; work with a clinician. Stop and reassess if you develop fever, worsening pain, or persistent diarrhea. Pregnant users should review with their obstetric clinician first.
Frequently asked questions
Is a high dose probiotic better than a low dose?
It depends on the job. High dose (around 100 billion CFU) is useful short term after antibiotics or infection. For steady, long-term maintenance, many do fine on lower doses. More is not always better if your symptoms are mild.
How long does a probiotic take to work?
For stool consistency and gas, expect 7–14 days. After antibiotics, give it 2–4 weeks. If nothing changes by a month, reassess strain choice, dose, or non-gut causes of symptoms with your clinician.
Can I take a probiotic with antibiotics?
Yes, separate them by 2–3 hours so the probiotic has a chance to survive. Start the probiotic on day one of antibiotics and continue for 2–4 weeks after finishing the prescription.
What side effects should I expect?
The most common are mild gas or bloating in the first few days as your microbiome adjusts. Taking with food and adequate hydration helps. Stop and seek care for fever, severe pain, or persistent diarrhea.
Do probiotics need refrigeration?
Follow the label. Some high dose probiotics are shelf-stable at room temperature if kept cool and dry, but last longer when refrigerated. Avoid heat exposure, car glove boxes, and bathroom humidity.
Is 100 billion CFU too much to start with?
Not if you’re recovering from antibiotics or a gut infection. If you’re new to probiotics or sensitive, you can start every other day for a week, then move to daily as tolerated.
Can probiotics help IBS symptoms?
They can help some people with loose stools, post-infectious IBS, or bloating, but responses vary. If symptoms persist, consider stool testing, breath testing for small intestinal bacterial overgrowth, or diet changes with a clinician.
Is a probiotic safe in pregnancy?
Generally considered safe for healthy pregnancies, but data by strain is limited. Review with your obstetric clinician, especially if you have risk factors like preterm labor history or significant immune issues.
How to take it & ingredients
Suggested use: Take 1 capsule per day or as recommended by your health care professional.
Active ingredients
1 capsule per serving · 30 servings
▼
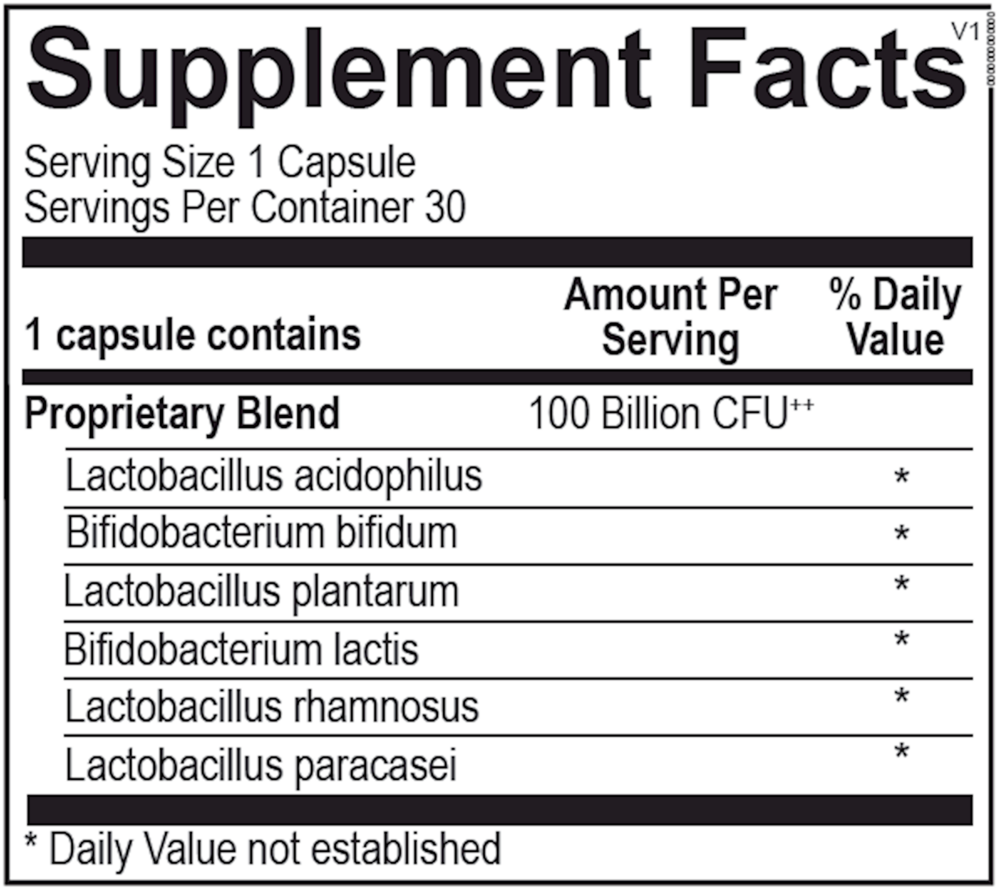
Proprietary Blend
100 billion CFU, 423 mg
Lactobacillus acidophilus (La-14)
-
Bifidobacterium bifidum (Bb-02)
-
Lactobacillus plantarum (Lp-115)
-
Bifidobacterium lactis (Bl-04)
-
Lactobacillus rhamnosus (Lr-32)
-
Lactobacillus paracasei (Lpc-37)
-
Other ingredients: Natural Vegetable Capsules, Microcrystalline Cellulose, Silicon Dioxide, Magnesium Stearate
Certifications
Benefits
Warnings
Customers also considered

Thorne
Bacillus Coagulans
60 capsules
$33.00
Add to cart for lower price

Thorne
Complete Biotic
30 packets
$46.00
Add to cart for lower price
Dr. Mercola
Complete Probiotics 70 Billion CFU
30 capsules
$37.99
Add to cart for lower price

SmartyPants
Digestive Probiotic & Prebiotic Grape
60 gummies
$36.99
Add to cart for lower price