
Ortho Molecular Products
Pro Bono® by Ortho Molecular Products
60 capsules
Comprehensive Calcium, Magnesium & Vitamin Blend for Bone and Overall Health$139.64
Purchase options
Practitioner-grade brand3rd-party testedFree shipping $50+
Gluten Free·Wheat Free·Yeast Free·Artificial Color Free·Artificial Flavor Free
Ortho Molecular Products Pro Bono® overview
If your DEXA scan shows low bone density and you want a non-drug option, strontium citrate for bone density paired with calcium, vitamin D3, and vitamin K2 is a practical stack. This blend fits postmenopausal women, men with age-related bone loss, adults on long-term steroids, and those with low dietary calcium. Check Vitamin D, 25-Hydroxy before starting; the built-in D3 here is a maintenance dose, so established deficiency usually needs higher D3 short term, then this for upkeep.
Strontium slows bone breakdown and nudges formation, which can raise DEXA readings within 6–12 months. The catch is that strontium sits in bone and can overestimate DEXA, so track fracture risk and bone turnover markers like CTX (bone resorption) and P1NP (bone formation), not the scan alone. Vitamin K2 MK-7 activates osteocalcin (the protein that locks calcium into bone) and Matrix Gla Protein (which helps keep calcium out of arteries). Calcium hydroxyapatite mirrors natural bone mineral, magnesium supports bone matrix, and boron helps vitamin D signaling.
Use two packets daily, morning and evening, with food. For best strontium uptake, separate it from calcium-rich meals or mineral supplements by about two hours. If you’re on levothyroxine (thyroid hormone) or quinolone/tetracycline antibiotics, separate this mineral-heavy formula by at least four hours to avoid binding. Recheck Vitamin D, 25-Hydroxy and, if available, CTX or P1NP after 3–6 months to gauge effect and adjust.
Vitamin K (K1 and K2) reduces the effect of warfarin and similar vitamin K–dependent anticoagulants, so skip this if you rely on those drugs unless your prescriber actively manages dosing and INR. Minerals in this formula can also interfere with absorption of bisphosphonates taken orally; take those medications at a different time of day per your clinician’s instructions.
Avoid in pregnancy due to added preformed vitamin A (palmitate) and uncertain strontium safety. Use caution if you form calcium kidney stones, have high blood calcium, sarcoidosis, or significant kidney disease. If your Omega-3 Index and hs-CRP (an inflammation marker) are high, address those risks separately; they matter for fracture risk but aren’t fixed by calcium alone.
Frequently asked questions
Should I take strontium citrate away from calcium?
Yes. Strontium and calcium compete for absorption. Take strontium at least two hours away from calcium-rich meals or supplements to improve uptake.
How long until I see bone changes on a DEXA scan?
Plan on 6–12 months before a meaningful change. Strontium can overstate DEXA increases, so also track CTX and P1NP and discuss fracture risk with your clinician.
Is vitamin K2 safe if I’m on a blood thinner?
Not with warfarin-type anticoagulants. Vitamin K counters their effect. If you’re on warfarin, avoid K2 unless your prescriber adjusts dosing and monitors INR closely.
Can I use this with alendronate or other osteoporosis drugs?
Often yes, but separate timing. Minerals can block absorption of oral bisphosphonates. Take the medication on an empty stomach as directed, then add minerals later.
Is 1,000 IU of vitamin D3 enough for bones?
It’s a maintenance dose. If your Vitamin D, 25-Hydroxy is low, you’ll usually need a higher dose short term under clinician guidance, then maintain with 1,000 IU.
Does strontium skew DEXA results?
It can. Strontium is heavier than calcium and can make DEXA look better than true mineral content. Use CTX/P1NP and clinical risk alongside DEXA to judge progress.
What side effects should I watch for?
Common issues are mild nausea or constipation from minerals. Taking with meals, splitting doses, extra fluids, and magnesium in the formula help. Stop if you get persistent GI upset.
Can men take this bone supplement?
Yes. Men with low bone density, especially with low dietary calcium or age-related loss, can benefit. Pair with resistance training and adequate protein for best results.
How to take it & ingredients
Suggested use: 2 packets per day, one AM packet in the morning and one PM packet in the evening or as recommended by your health care professional. Maintenance: 1 packet per day, alternating one AM packet on odd days and one PM packet on even days or as recommended by your health care professional.
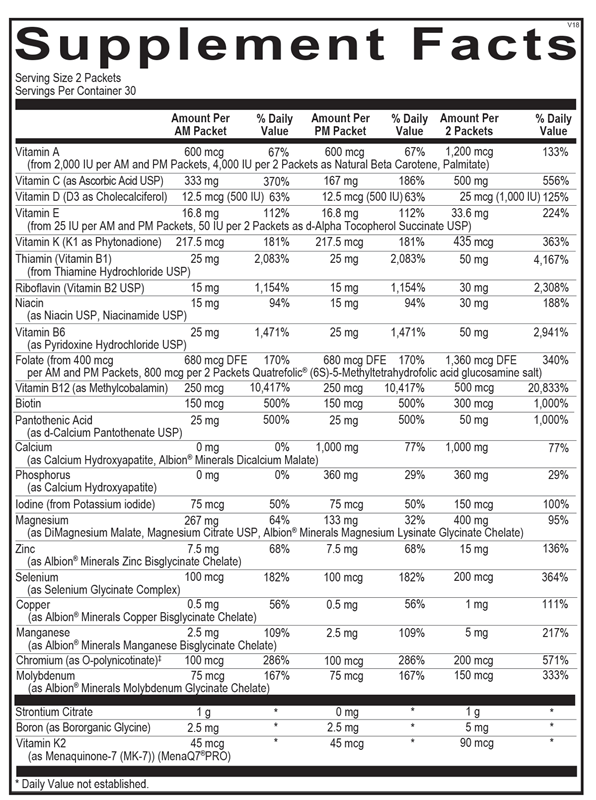
Active ingredients
2 packets per serving
Vitamin A
From Natural Beta Carotene and Palmitate (4,000 IU per 2 packets)
From Natural Beta Carotene and Palmitate (4,000 IU per 2 packets)
1200 mcg
Strontium Citrate
500 mg
Boron
As Bororganic Glycine
As Bororganic Glycine
5 mg
Vitamin K
K1 as Phytonadione; K2 as Menaquinone-7 (MK-7) (MenaQ7®PRO)
K1 as Phytonadione; K2 as Menaquinone-7 (MK-7) (MenaQ7®PRO)
435 mcg, 90 mcg (K2)
Vitamin C
As Ascorbic Acid USP
As Ascorbic Acid USP
50 mg
Vitamin D
D3 as Cholecalciferol
D3 as Cholecalciferol
25 mcg, 1000 IU
Vitamin E
As d-Alpha Tocopherol Succinate USP (50 IU per 2 packets)
As d-Alpha Tocopherol Succinate USP (50 IU per 2 packets)
50 IU
Thiamin (Vitamin B1)
From Thiamine Hydrochloride USP
From Thiamine Hydrochloride USP
25 mg
Riboflavin (Vitamin B2)
USP
USP
15 mg
Vitamin B6
As Pyridoxine Hydrochloride USP
As Pyridoxine Hydrochloride USP
25 mg
Niacin
As Niacin USP, Niacinamide USP
As Niacin USP, Niacinamide USP
15 mg
Folate
From Quatrefolic® (6S)-5-Methyltetrahydrofolic acid glucosamine salt
From Quatrefolic® (6S)-5-Methyltetrahydrofolic acid glucosamine salt
1360 mcg DFE
Vitamin B12
As Methylcobalamin
As Methylcobalamin
500 mcg
Biotin
300 mcg
Calcium
As Calcium Hydroxyapatite, Albion® Minerals Dicalcium Malate
As Calcium Hydroxyapatite, Albion® Minerals Dicalcium Malate
1000 mg
Phosphorus
As Calcium Hydroxyapatite
As Calcium Hydroxyapatite
360 mg
Pantothenic Acid
As d-Calcium Pantothenate USP
As d-Calcium Pantothenate USP
50 mg
Iodine
From Potassium Iodide
From Potassium Iodide
150 mcg
Magnesium
As DiMagnesium Malate, Magnesium Citrate USP, Albion® Minerals Magnesium Lysinate Glycinate Chelate
As DiMagnesium Malate, Magnesium Citrate USP, Albion® Minerals Magnesium Lysinate Glycinate Chelate
400 mg
Chromium
As O-polynicotinate (ChromeMate®)
As O-polynicotinate (ChromeMate®)
200 mcg
Zinc
As Albion® Minerals Zinc Bisglycinate Chelate
As Albion® Minerals Zinc Bisglycinate Chelate
15 mg
Selenium
As Selenium Glycinate Complex
As Selenium Glycinate Complex
200 mcg
Copper
As Albion® Minerals Copper Bisglycinate Chelate
As Albion® Minerals Copper Bisglycinate Chelate
1 mg
Molybdenum
As Albion® Minerals Molybdenum Glycinate Chelate
As Albion® Minerals Molybdenum Glycinate Chelate
150 mcg
Manganese
As Albion® Minerals Manganese Bisglycinate Chelate
As Albion® Minerals Manganese Bisglycinate Chelate
5 mg
Other ingredients: Hypromellose (Natural Vegetable Capsules), Microcrystalline Cellulose, Magnesium Stearate, Silicon Dioxide
Certifications
Benefits
Warnings
Customers also considered

AlgaeCal Inc.
AlgaeCal Plus
120 capsules
$81.99extra 20% off with Subscribe & Save
New Chapter
Bone Strength Take Care
60 tablets
$40.99extra 20% off with Subscribe & Save

Pure Encapsulations
Magnesium Citrate
180 capsules
$34.50extra 19% off with Subscribe & Save

Ortho Molecular Products
OsteoBase
90 capsules
$39.68extra 10% off with Subscribe & Save