
Pure Encapsulations
Potassium Citrate 200 mg by Pure Encapsulations
90 capsules · 90-day supply
Essential Mineral for Electrolyte Balance and Muscle Function$18.50
Purchase options
Practitioner-grade brand3rd-party testedFree shipping $50+
Vegan·Vegetarian·Gluten Free
Pure Encapsulations Potassium Citrate overview
If you get leg cramps after sweaty workouts or your Potassium on a Basic Metabolic Panel runs low-normal, potassium citrate is a practical bump from diet-sized doses. It’s also useful if your 24-hour urine shows low citrate or acidic urine pH, two patterns linked to calcium oxalate kidney stones. The total here is a maintenance-level intake, not a therapeutic dose for stone prevention or marked deficiency.
Potassium drives electrical signaling in nerves and muscles, including steady heart rhythm. The citrate form matters: citrate acts as an alkali, raising urine pH and binding free calcium, which lowers the tendency for calcium oxalate crystals to form. Higher potassium intake also helps the kidneys excrete sodium, a reason many adults see small drops in blood pressure within a few weeks.
Take two small doses daily with food, as the label suggests, to limit stomach upset. Dividing morning and evening works well. Expect blood pressure effects within 2 to 4 weeks and urine chemistry changes within days, confirmed on a 24-hour urine or spot Urine pH. If you need more than a gentle increase, your clinician may use higher mEq prescriptions and recheck labs.
Skip this or use only with clinician oversight if you have chronic kidney disease, high baseline Potassium, or take drugs that raise potassium: ACE inhibitors (like lisinopril), ARBs (like losartan), potassium‑sparing diuretics (spironolactone, eplerenone, amiloride, triamterene), high-dose NSAIDs, or trimethoprim. Monitor Potassium, Creatinine, and eGFR after changes. Avoid stacking with potassium-based salt substitutes.
Frequently asked questions
What is potassium citrate used for?
Main uses are topping up low-normal potassium, modest blood pressure reduction when sodium intake is high, and alkalinizing urine to reduce calcium oxalate stone risk. It’s maintenance-level here, not a prescription-strength stone therapy.
Does potassium citrate help kidney stones?
Yes for calcium oxalate stones if your urine citrate is low or urine is acidic. It raises urinary citrate and pH. The dose in this supplement is gentle; stone prevention often uses higher mEq dosing prescribed and monitored with 24-hour urine.
How long does potassium citrate take to work?
Urine pH and citrate shifts occur within days, seen on 24-hour urine or dipstick pH. Blood pressure changes, when they happen, usually appear within 2–4 weeks alongside reduced sodium intake.
Can I take potassium citrate with blood pressure medication?
It depends. Avoid unsupervised use with ACE inhibitors or ARBs because combined effects can raise potassium too high. If you’re on thiazide diuretics, your clinician may allow it but will check Potassium and Creatinine.
What side effects should I watch for?
Upset stomach, nausea, or loose stools are the most common, improved by taking with meals. High potassium can cause weakness, tingling, or abnormal heart rhythm—seek care if these occur, especially if you have kidney disease.
Can I open the capsule and mix it with food?
Yes, you can open and mix with water or a small snack. The citrate tastes tart. Always take with food and a full glass of water to reduce stomach irritation.
Is potassium citrate safe in pregnancy?
Generally, potassium from food and standard supplements is safe in healthy pregnancies, but any potassium supplement should be cleared with your obstetric clinician, especially if you have hypertension or kidney issues.
Do I need labs before taking potassium citrate?
If you’re healthy with normal kidney function, routine labs aren’t mandatory, but checking Potassium and Creatinine once is prudent. With kidney disease or interacting drugs, get Potassium, Creatinine, eGFR, and consider 24-hour urine if using for stones.
How to take it & ingredients
Suggested use: Take 2 capsules daily in divided doses with meals or as directed by a healthcare professional.
Active ingredients
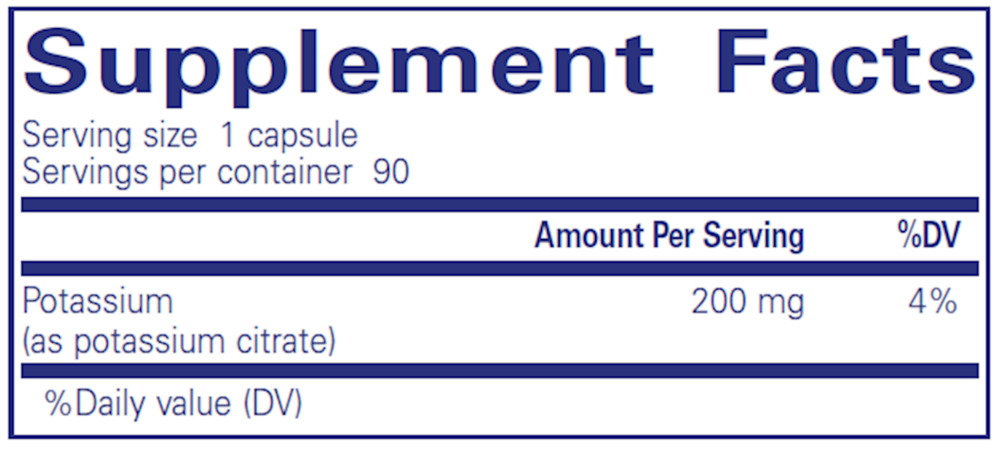
1 capsule per serving · 90 servings
Potassium
Potassium Citrate
Potassium Citrate
200 mg
Other ingredients: Ascorbyl palmitate, Vegetarian capsule (cellulose, water)
Certifications
Benefits
Warnings