



Thorne
Vitamin B12 by Thorne
60 capsules · 60-day supply
Essential Vitamin B12 for Energy, Mood, and Cognitive Support$XX.XX$24.00retail
Purchase option
21% below MSRP3rd-party tested for purity & potencyFree shipping $50+
Gluten Free·Soy Free·Dairy Free·Milk Free
Thorne Vitamin B12 overview
If you’re low on energy, eat little or no animal protein, or your Vitamin B12 blood test runs low-normal, methylcobalamin vitamin B12 is the straightforward fix. It’s a strong fit for vegans and vegetarians, people on metformin or acid-reducing meds, and anyone with elevated Homocysteine (an amino acid that rises when B12 or folate is lacking) or high Methylmalonic Acid, MMA (a marker that climbs when cells are short on B12). If your deficiency is established or you’ve had bariatric surgery, you can still use high-dose oral B12, but do it with clinician guidance and plan on rechecking labs within 4–12 weeks.
Methylcobalamin is an “active” vitamin B12 form your cells can use as-is, so it doesn’t require the conversion step cyanocobalamin needs. In the brain and nerves it donates methyl groups (the small chemical tags used to make neurotransmitters and maintain myelin, the insulation on nerves). In the bloodstream it helps turn homocysteine back into methionine, which is why Homocysteine often falls within 4–8 weeks. It also helps convert odd-chain fats into energy, reflected by a drop in MMA when cells are replete.
The suggested use is one capsule up to three times per day. Take methylcobalamin with or without food; morning or midday suits most people because B12 can feel energizing. If your Vitamin B12 or MMA is low, daily use at this strength is a practical repletion strategy, then taper to a maintenance schedule once labs normalize. Folate and vitamin B6 help with homocysteine recycling, but avoid mega-dosing folic acid without checking labs.
Severe numbness, balance issues, or known pernicious anemia (autoimmune loss of intrinsic factor, the gut carrier for B12) warrant medical care and often prescription-strength B12. After gastric bypass, absorption is unpredictable—use high-dose oral methylcobalamin under supervision and verify with Vitamin B12, MMA, and Homocysteine. If you’ve had recent nitrous oxide anesthesia (which inactivates B12), contact your clinician promptly. History of cobalt allergy or unexplained acne flares with B12 are reasons to avoid or reduce the dose.
How fast will I feel it? If low, many notice steadier energy within 1–2 weeks, with Homocysteine and MMA improving by 4–8 weeks. Is methylcobalamin better than cyanocobalamin? It’s already in an active form and is well-tolerated; both can replete B12, but this avoids the conversion step. Do I need folate with it? Only if labs or diet suggest low folate; overshooting folic acid can hide a B12 problem, so test and personalize.
Frequently asked questions
Is methylcobalamin better than cyanocobalamin?
Both raise B12, but methylcobalamin is already in an active form your cells use directly. It’s well-tolerated and avoids a conversion step. Cyanocobalamin works too and is cheaper; choice often comes down to tolerance, preference, and clinician guidance.
How long does vitamin B12 take to work?
Energy and mood can improve within 1–2 weeks if you were low. Lab markers move on a set timeline: MMA often drops in 1–3 weeks, Homocysteine in 4–8 weeks, and red blood cell changes on a CBC take several weeks to fully normalize.
Can I take vitamin B12 at night?
You can, but many prefer morning or midday because B12 can feel stimulating. If you notice vivid dreams or trouble falling asleep, shift the dose earlier. It’s fine with or without food.
Who is most at risk for low B12?
Vegans and vegetarians, adults over 60, people on metformin or acid-suppressing drugs, and those with bariatric surgery are common. If you’re in these groups, check Vitamin B12, MMA, and Homocysteine and supplement as needed.
Does B12 interact with medications like metformin or PPIs?
Metformin and acid-reducing drugs (PPIs and H2 blockers) reduce B12 absorption over time. Supplementing methylcobalamin can offset this, but confirm with labs. There’s no known harmful drug interaction from taking B12 itself.
Are there side effects from high-dose B12?
B12 is water-soluble and generally safe. A small minority notice acne, flushing, or anxiety-like restlessness at higher doses; lowering the dose usually fixes it. True allergy is rare but possible in cobalt-sensitive individuals.
Do I need adenosylcobalamin as well as methylcobalamin?
Most people replete fine with methylcobalamin alone. Adenosylcobalamin is another active B12 form used in mitochondria; combination products exist, but evidence that both are required orally for repletion is limited.
Will B12 lower my homocysteine by itself?
If your homocysteine is high due to low B12, methylcobalamin often lowers it in 4–8 weeks. If folate or vitamin B6 is also low, you may need those too. Test first to target the right nutrient.
How to take it & ingredients
Suggested use: Take 1 capsule one to three times daily or as recommended by your health professional.
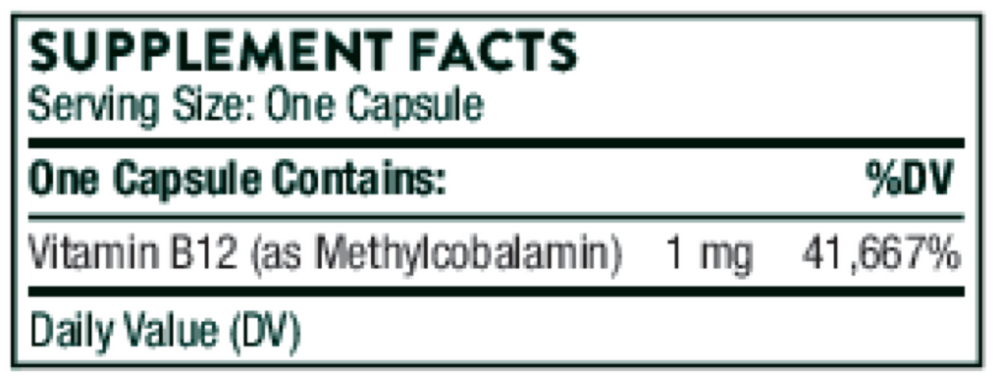
Active ingredients
1 capsule per serving · 60 servings
Vitamin B12
Methylcobalamin
Methylcobalamin
1000 mcg, 1 mg
Other ingredients: Hypromellose Capsule, Leucine, Microcrystalline Cellulose, Silicon Dioxide
Certifications
Benefits
Warnings


