

Biotics Research
Methyfolate Plus by Biotics Research
120 tablets · 240-day supply
Essential Folate and B12 for Optimal Energy and Cellular Health$XX.XX$28.99retail
This item is currently out of stockGet notified when this item is back in stock
21% below MSRP3rd-party tested for purity & potencyFree shipping $50+
Gluten Free·Dairy Free·Milk Free
Biotics Research Methyfolate Plus overview
If you’ve been told you carry an MTHFR variant and are searching for methylfolate for MTHFR, this low, steady dose fits maintenance rather than heavy repletion. It’s a good pick if your Folate and Vitamin B12 labs are in the lower normal range, your homocysteine (an amino acid tied to vascular risk) runs high-normal, or you feel better on methylated B vitamins. Vegans and long‑term acid‑suppressor users often sit on the edge of B12 insufficiency, so pairing methylfolate with methylcobalamin makes sense here.
Methylfolate is the active form of folate that your cells actually use, so it doesn’t rely on MTHFR conversion. Together with methylcobalamin (vitamin B12 in its co‑enzyme form), it remethylates homocysteine back to methionine, fueling methylation (the cell’s on/off tagging system for DNA and neurotransmitters). In practice, that pathway is why many see homocysteine fall within 4–12 weeks when folate and B12 are adequate, especially if riboflavin (vitamin B2) and vitamin B6 are also sufficient. This is nutrient tuning, not an antidepressant replacement.
Biotics Research suggests half a tablet daily, which is a gentle, maintenance‑level intake. Take it in the morning with food if B vitamins make you queasy, or without food if you tolerate them well. If you’re sensitive to stimulatory feelings from methyl donors, start every other day for a week, then move to daily. If your homocysteine is meaningfully high, a higher folate/B12 plan or a full B‑complex is usually more effective; re‑test labs in 8–12 weeks.
High folate can mask a vitamin B12 deficiency by normalizing anemia while nerve damage progresses, so check Vitamin B12 and Methylmalonic Acid (the backup marker that rises when B12 is low) if you have numbness, tingling, or long‑term vegan intake. If you take methotrexate for cancer or autoimmune disease, or anti‑seizure drugs like valproate or carbamazepine, talk to your clinician before adding methylfolate. Pregnancy needs a prenatal‑level folate dose and iodine, so use a dedicated prenatal rather than this maintenance formula.
Frequently asked questions
What does methylfolate do in the body?
Methylfolate is the active form of folate that, with vitamin B12, converts homocysteine back to methionine. That supports methylation, a control system your cells use for DNA repair and neurotransmitter balance. It’s about nutrient adequacy, not a quick mood fix.
How long does methylfolate take to lower homocysteine?
Most responders see movement within 4–12 weeks once folate and B12 are adequate. If homocysteine barely changes, check vitamin B2 and B6 status, thyroid function, kidney health, alcohol intake, and dose; sometimes a higher folate/B12 plan or full B‑complex is needed.
Is methylfolate better than folic acid?
For people with reduced MTHFR activity, methylfolate bypasses a conversion step and is more direct. For others, both can replete folate. Clinically, methylfolate avoids unmetabolized folic acid in blood and is often chosen when homocysteine is a goal marker.
Is 400 mcg of methylfolate enough?
It’s a maintenance dose if your Folate is low‑normal and you’re steady on labs. For established deficiency or clearly elevated homocysteine, higher folate paired with B12 (and sometimes B6 and riboflavin) is typically used short‑term, then you step down and re‑test.
Can methylfolate cause anxiety or insomnia?
Some people feel wired, headachy, or irritable at first, especially with larger methyl doses. Start low, take it in the morning, and increase gradually. If sensitivity persists, consider adding magnesium or using every other day while you reassess dose and B‑complex balance.
Can methylfolate hide a B12 deficiency?
Yes. Folate can fix anemia while B12‑related nerve damage continues. If you’re older, vegan, or have numbness or balance issues, check Vitamin B12 and Methylmalonic Acid before and during folate use, and include methylcobalamin to keep B12 replete.
Is methylfolate safe in pregnancy?
Folate is essential in pregnancy, but use a prenatal that provides the full folate amount plus iron, iodine, choline, and DHA. This maintenance‑level methylfolate isn’t a complete prenatal solution. Ask your obstetric clinician which form and dose they prefer.
Does methylfolate interact with methotrexate or seizure meds?
It can. Methotrexate and some anticonvulsants affect folate pathways, so adding methylfolate without guidance can change drug effects. Do not start without your prescribing clinician’s input if you use methotrexate, valproate, carbamazepine, or phenytoin.
How to take it & ingredients
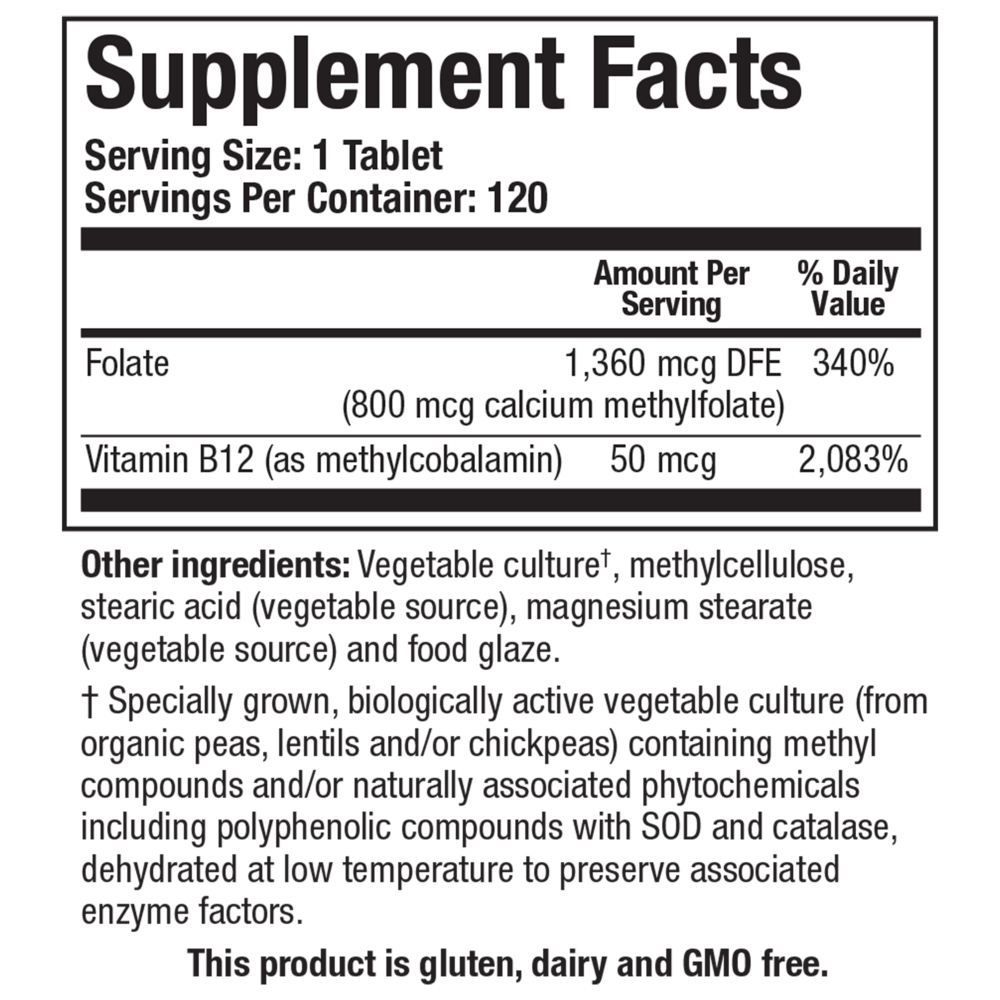
Suggested use: Take half a tablet daily, or as directed by your healthcare professional.
Active ingredients
0.5 tablets per serving · 240 servings
Folate
Calcium Methylfolate
Calcium Methylfolate
400 mcg, 680 mcg DFE
Vitamin B12
Methylcobalamin
Methylcobalamin
25 mcg
Other ingredients: Vegetable culture† (rich in polyphenolic compounds with SOD and catalase activity), Methylcellulose, Stearic acid (vegetable source), Magnesium stearate (vegetable source), Food glaze
Certifications
Benefits
Warnings
Customers also considered

Theralogix
ConceptionXR Reproductive Health Formula
180 tablets
$XX.XX$77.99retail
Add to cart to see your price

Pure Encapsulations
Folate 1000
90 capsules
$XX.XX$34.50retail
Add to cart to see your price

Pure Encapsulations
Folate 400
90 capsules
$XX.XX$22.00retail
Add to cart to see your price

MethylPro
L-Methylfolate 5 mg
30 capsules
$XX.XX$18.99retail
Add to cart to see your price