

MethylPro
L-Methylfolate 5 mg by MethylPro
30 capsules · 30-day supply
Bioactive Folate for Optimal Methylation and Energy Support$18.99
Purchase options
Practitioner-grade brand3rd-party testedFree shipping $50+
Vegetarian·Gluten Free·Soy Free·Dairy Free·Egg Free·Fish Free·
MethylPro L-Methylfolate 5 mg overview
This is for adults who need active folate repletion, not just maintenance. L-methylfolate 5 mg fits if your Folate is low, Homocysteine is elevated (a breakdown product that rises when methylation is sluggish), or you have an MTHFR variant and haven’t felt well on folic acid. It’s also considered after bariatric surgery, with alcohol overuse, or with long-term antiepileptics, which can lower folate. If you’re targeting mood, psychiatrists often trial higher doses; 5 mg is a conservative start.
L-methylfolate is the body-ready form of folate that bypasses MTHFR (the enzyme that activates folic acid). It donates methyl groups that convert homocysteine back to methionine, raising SAMe (the universal methyl donor used to make neurotransmitters like serotonin and dopamine). This is why it lowers Homocysteine and why higher doses have been studied as an add-on in depression. Unlike folic acid, it doesn’t create unmetabolized folic acid in the blood.
Take one capsule daily, with or without food. L-methylfolate can feel energizing; many prefer morning. If you’re sensitive or new to methyl donors, consider starting with a lower dose on alternate days and working up within 1–2 weeks. Pairing with Vitamin B12 testing (and repleting B12 if low) prevents masking B12-related anemia. Expect Homocysteine changes within 4–12 weeks, then recheck labs.
Check Vitamin B12 and Methylmalonic Acid first; high-dose folate can normalize blood counts while B12-related nerve injury worsens. Use clinician guidance if pregnant or trying to conceive, if you’ve had colorectal polyps or cancer, or if you’re on methotrexate for autoimmune disease (folate can counter its effect; dosing needs coordination). Report agitation, anxiety, headaches, or insomnia—reduce dose or pause if they appear.
Frequently asked questions
What’s the difference between L-methylfolate and folic acid?
L-methylfolate is the active form your cells use directly. Folic acid must be converted by MTHFR first, which is less efficient in many people. L-methylfolate also avoids unmetabolized folic acid in the bloodstream.
How long does L-methylfolate 5 mg take to work?
For Homocysteine, expect movement within 4–12 weeks, then recheck labs. For mood uses, trials with higher doses evaluate response over 4–8 weeks; with 5 mg, give it several weeks before judging.
Can L-methylfolate mask a B12 deficiency?
Yes. High-dose folate can correct anemia while B12-related nerve damage progresses. Check Vitamin B12 and Methylmalonic Acid before starting and replete B12 if low or borderline.
Is L-methylfolate safe in pregnancy?
Use only with clinician guidance. Needs are higher in some pregnancies, but 5 mg is a therapeutic dose. Your prenatal typically uses lower folate; dosing above that should be individualized.
Does L-methylfolate interact with methotrexate?
It can. L-methylfolate may reduce the intended effect of low-dose methotrexate for autoimmune disease. Any folate with methotrexate should be coordinated with your prescriber.
What side effects should I watch for?
The most common are restlessness, anxiety, headaches, nausea, or insomnia. If they occur, lower the dose, take in the morning, or pause and speak with your clinician.
Can I take L-methylfolate with antidepressants?
Some psychiatrists add higher-dose L-methylfolate to antidepressants. If you’re on an SSRI or SNRI, discuss dose and timing with your prescriber rather than self-adjusting.
Do I need other tests with L-methylfolate?
Yes. Folate, Vitamin B12, Methylmalonic Acid, and Homocysteine are useful. If labs are low or high, correct B12 first or alongside folate, then recheck after 4–12 weeks.
How to take it & ingredients
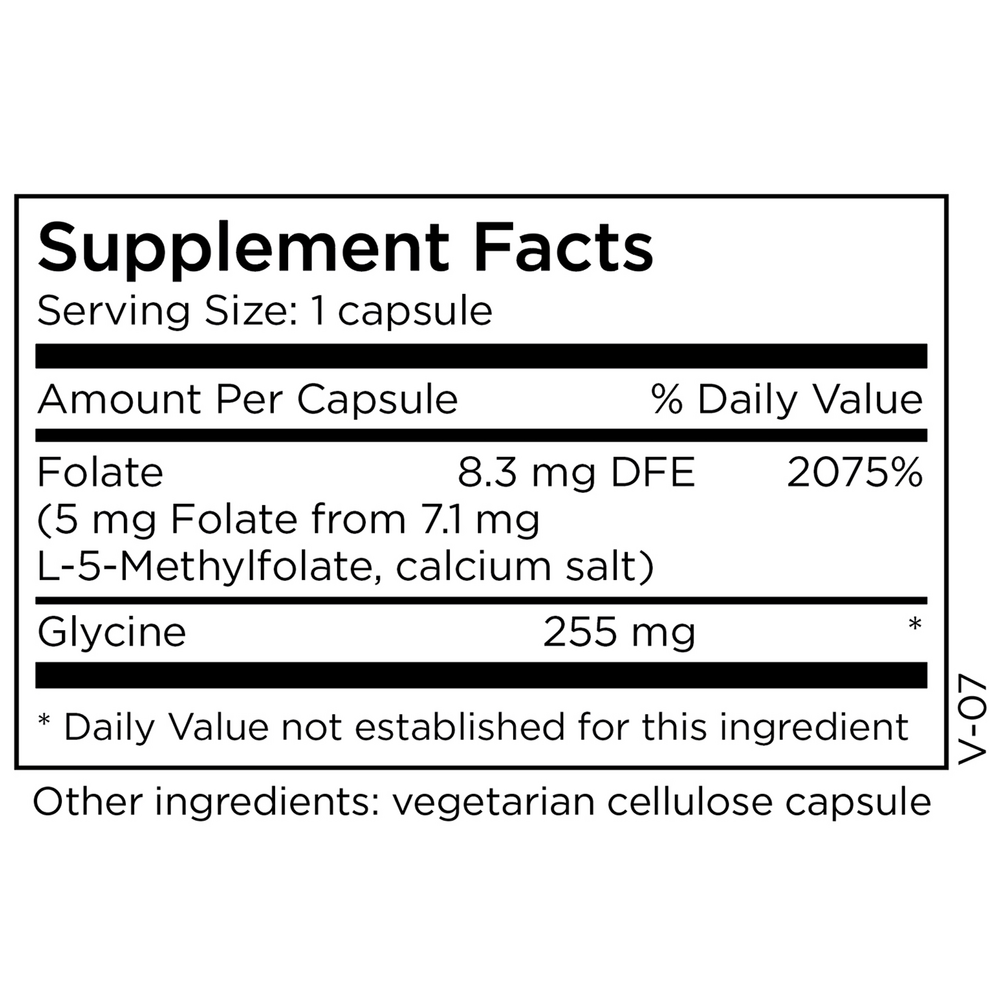
Suggested use: Take one capsule per day or as directed by a healthcare professional.
Active ingredients
1 capsule per serving · 30 servings
Folate
L-5-Methylfolate, calcium salt
L-5-Methylfolate, calcium salt
5 mg, 8.3 mg DFE
Glycine
255 mg
Other ingredients: Vegetarian cellulose capsule
Certifications
Benefits
Warnings
Customers also considered

Theralogix
ConceptionXR Reproductive Health Formula
180 tablets
$77.99extra 21% off with Subscribe & Save

Pure Encapsulations
Folate 1000
90 capsules
$34.50extra 19% off with Subscribe & Save

Pure Encapsulations
Folate 400
90 capsules
$22.00extra 18% off with Subscribe & Save

NuMedica
Methyl Folate
120 capsules
$37.99extra 21% off with Subscribe & Save