

NuMedica
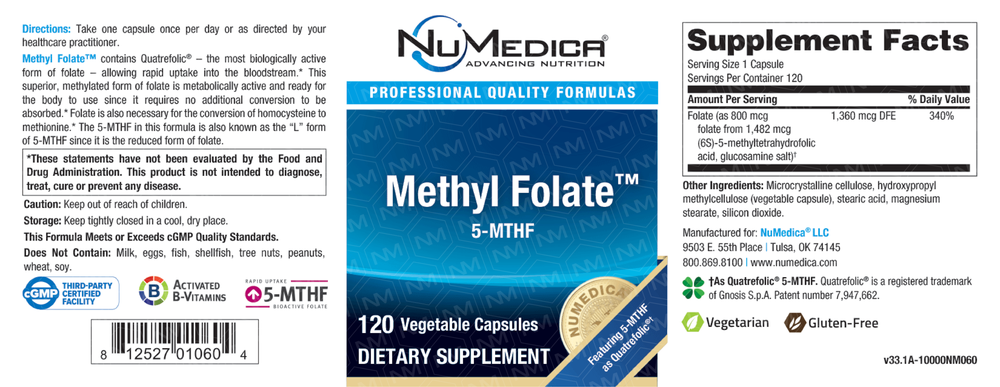
Methyl Folate 800 mcg (1360 mcg DFE) by NuMedica
120 capsules · 120-day supply
Bioactive Folate for Enhanced Energy and Cognitive Support$37.99
Purchase options
Practitioner-grade brand3rd-party testedFree shipping $50+
Vegetarian·Gluten Free·Soy Free·Egg Free·Milk Free·Tree Nut Free·
NuMedica Methyl Folate overview
If your Folate or RBC Folate is low, or your Homocysteine (an amino acid tied to heart and brain aging) runs high, methyl folate is the right form to correct it. It’s useful if you have common MTHFR gene variants that slow folic acid activation, drink alcohol regularly, or eat few leafy greens. This 800 mcg dose suits maintenance or mild deficiency; with clearly low labs or very high Homocysteine, clinicians often pair methyl folate with Vitamin B12, Vitamin B6, and riboflavin and retest within 4 to 8 weeks.
Methyl folate (L-5-MTHF) is the active folate your cells use for methylation, the chemical tagging system that turns genes on and off and builds neurotransmitters. Unlike folic acid, which must be converted by the MTHFR enzyme, L-5-MTHF is already in the end form and gets to work quickly. It donates a methyl group to homocysteine to form methionine, which helps lower Homocysteine on labs and supports DNA synthesis and red blood cell formation. NuMedica uses Quatrefolic, a stabilized glucosamine salt that’s well absorbed.
Take one capsule daily, with or without food. Morning works best for many since methyl folate can feel energizing. If you’ve had low Vitamin B12 or borderline Methylmalonic Acid (a marker of B12 function), add B12 alongside to avoid masking a B12 deficiency. For elevated Homocysteine, expect changes on repeat labs in 4 to 8 weeks. If you need higher repletion, a clinician may temporarily use a larger dose, then step back to 800 mcg for upkeep.
Don’t start methyl folate if you have untreated Vitamin B12 deficiency, pernicious anemia, or unexplained anemia—correct B12 first. Use clinician guidance if you take methotrexate (folate antagonists), antiepileptics (like valproate or carbamazepine), or have a history of bipolar disorder, since activation can worsen agitation. If you’re pregnant or planning, folate is essential, but coordinate the exact dose and form with your prenatal plan and repeat Folate and Homocysteine testing.
Frequently asked questions
Should I take methyl folate or folic acid?
If you have MTHFR variants, elevated Homocysteine, or low Folate on labs, methyl folate is more reliable because it’s already in the active form. Folic acid needs conversion before use, which is slower in many people. Use methyl folate especially when you want a predictable lab response.
How long does methyl folate take to lower homocysteine?
Most see Homocysteine improve within 4–8 weeks. The timeline is faster when Vitamin B12, Vitamin B6, and riboflavin status are adequate, and slower with ongoing alcohol use or hypothyroidism. Recheck Homocysteine after one to two months to confirm response.
Can I take methyl folate with Vitamin B12?
Yes, and it’s often smart. Folate can “normalize” anemia from B12 deficiency without fixing nerve risk, so pairing methyl folate with B12 (and checking Vitamin B12 or Methylmalonic Acid) is prudent, especially for vegans, metformin users, and older adults.
Is methyl folate safe during pregnancy?
Folate is critical in pregnancy, but coordinate dose and form with your prenatal clinician. Many prenatals now use methyl folate. Verify your Folate and Homocysteine and avoid stacking extra products that push total folate intake higher than intended.
What are common methyl folate side effects?
Some feel jittery, anxious, or get headaches or insomnia at first, especially at higher doses. Try morning dosing, reduce the dose, or add B12 and magnesium. If agitation persists, pause and discuss with your clinician.
Does methyl folate interact with methotrexate or seizure meds?
It can. Folate can counter methotrexate’s effects, so only use under clinician guidance. Some antiepileptics alter folate metabolism; changing folate status can affect seizure control. Coordinate any changes with your prescribing doctor.
How much methyl folate should I take with an MTHFR mutation?
Many do well at 400–800 mcg daily, but needs vary. Start at 400–800 mcg, ensure adequate B12, and track Homocysteine and Folate after 4–8 weeks. Your clinician may adjust based on labs and symptoms.
How to take it & ingredients
Suggested use: Take one capsule daily or as directed by your healthcare practitioner.
Active ingredients
1 capsule per serving · 120 servings
Folate
6S-5-Methyltetrahydrofolic Acid, Glucosamine Salt
6S-5-Methyltetrahydrofolic Acid, Glucosamine Salt
800 mcg, 1360 mcg DFE
Other ingredients: Hydroxypropyl methylcellulose (vegetable capsule), Rice flour, Magnesium stearate, Stearic acid, Silica
Certifications
Benefits
Warnings
Customers also considered

Theralogix
ConceptionXR Reproductive Health Formula
180 tablets
$77.99extra 21% off with Subscribe & Save

Pure Encapsulations
Folate 1000
90 capsules
$34.50extra 19% off with Subscribe & Save

Pure Encapsulations
Folate 400
90 capsules
$22.00extra 18% off with Subscribe & Save

MethylPro
L-Methylfolate 5 mg
30 capsules
$18.99extra 21% off with Subscribe & Save