

Integrative Therapeutics
Berberine 500 mg by Integrative Therapeutics
120 capsules · 120-day supply
Supports Healthy Metabolism and Blood Sugar Levels$63.99
Purchase options
Practitioner-grade brand3rd-party testedFree shipping $50+
Vegan·Vegetarian·Gluten Free·Soy Free·Dairy Free·Milk Free·
Integrative Therapeutics Berberine overview
If you’re looking at berberine for blood sugar, this 500 mg capsule fits adults with mildly elevated glucose who want a non-drug nudge alongside diet and exercise. It’s a reasonable add-on if your Hemoglobin A1c (the 3‑month average of blood sugar), fasting glucose, or fasting insulin run high, or if triglycerides are elevated. I also use it in insulin-resistant patterns like PCOS when the Omega-3 Index and activity are already addressed. If your A1C is markedly high, berberine is not a substitute for prescriptions.
Berberine activates AMPK, the cell’s fuel gauge that tells tissues to pull sugar from the blood and burn fat. That shift reduces how much glucose the liver makes overnight and improves insulin sensitivity, which is why A1C often drops over 8 to 12 weeks. It also slows some carb breakdown in the gut and modestly improves blood lipids, with triglycerides and non‑HDL cholesterol often moving in the right direction. In practice, some patients see small ALT (a liver enzyme) improvements when fatty liver is present.
Integrative Therapeutics recommends 1 capsule two to three times daily. I prefer splitting doses with meals to blunt post‑meal glucose and reduce stomach upset. Expect fasting glucose to improve within 2 to 4 weeks, with Hemoglobin A1c and triglycerides shifting by 8 to 12 weeks. If you’re targeting weight, combine berberine with higher‑protein meals and resistance training; average weight change alone is modest over 3 months.
Pairing berberine with metformin, sulfonylureas, or insulin can overshoot blood sugar—monitor and involve your prescriber. It can raise levels of drugs cleared by P‑glycoprotein (the pump that moves drugs out of cells) or the CYP3A4 liver enzyme; cyclosporine, tacrolimus, and some statins are examples. Separate from other meds by 2–3 hours. Skip in pregnancy or while breastfeeding due to newborn bilirubin risks. Common side effects are nausea, constipation, or loose stools, which usually ease with meal‑time dosing.
Frequently asked questions
Does berberine really lower blood sugar?
Yes. Across randomized trials, berberine typically lowers Hemoglobin A1c by about 0.5–1.0% and reduces fasting glucose within 2–4 weeks. Effects are stronger when paired with diet, movement, and weight loss. It’s not a replacement for prescribed diabetes medications when A1C is significantly elevated.
How long does berberine take to work?
You’ll often see fasting glucose move in 2–4 weeks, with full effects on Hemoglobin A1c and triglycerides showing by 8–12 weeks. Keep the dose consistent and recheck labs after 8–12 weeks to judge response.
What is the best time to take berberine?
Take it with meals, split two to three times daily. Meal‑time dosing blunts post‑meal glucose and minimizes stomach upset. If you only dose twice, choose the two largest meals.
Can I take berberine with metformin?
Often, yes—but monitor closely. The combo can push blood sugar lower than expected. Track home readings, watch for dizziness or shakiness, and ask your prescriber if medication doses need adjustment.
Does berberine help with weight loss?
A little. Average weight change is modest over 8–12 weeks, but it can reduce waist circumference when insulin resistance is present. Pair it with higher‑protein diets and resistance training for a meaningful effect.
What are berberine’s side effects?
The most common are digestive—nausea, constipation, or diarrhea—especially if taken on an empty stomach. Taking it with meals and splitting doses usually fixes this. Rarely, people report headache or a drop in blood pressure.
Who should avoid berberine?
Avoid during pregnancy and breastfeeding due to risks to newborns. Use caution if you’re on cyclosporine, tacrolimus, certain statins, or strong blood‑sugar–lowering drugs. If you have liver or kidney disease, involve your clinician and monitor labs.
How to take it & ingredients
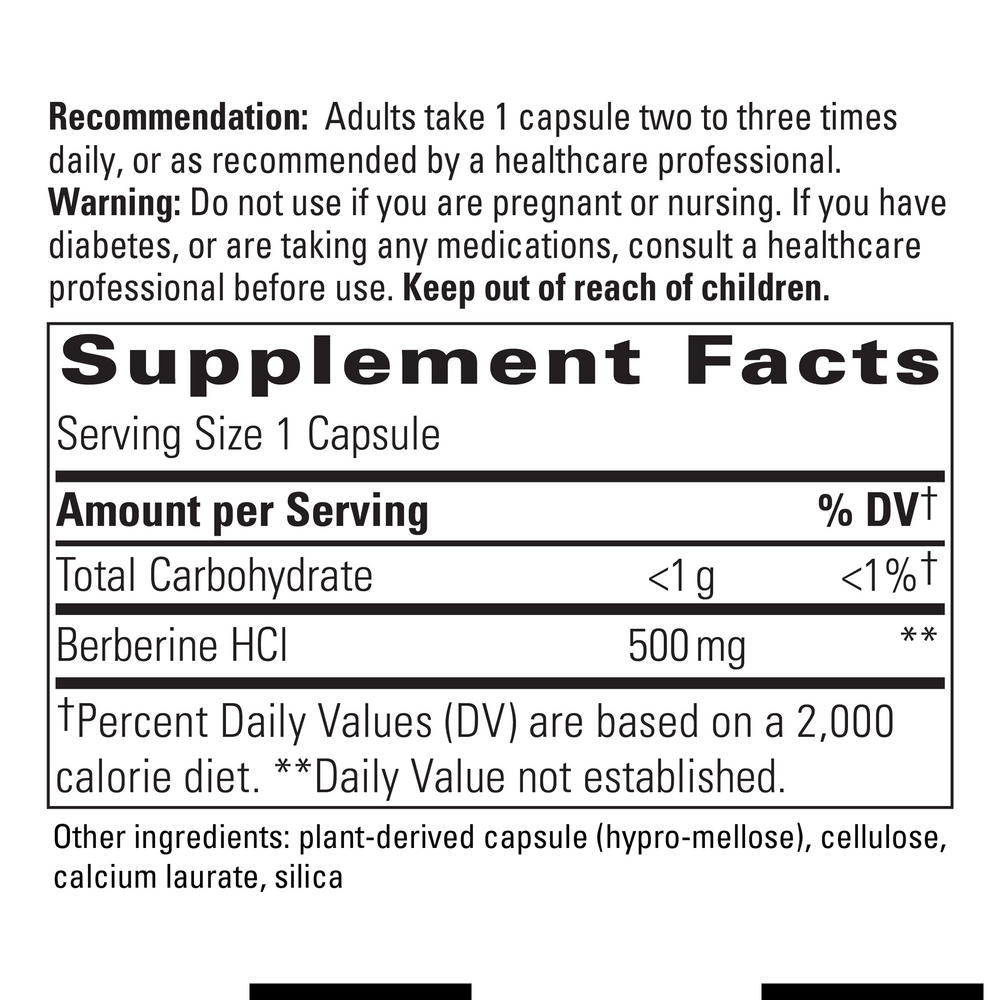
Suggested use: Take 1 capsule two to three times daily, or as recommended by your healthcare professional.
Active ingredients
1 capsule per serving · 120 servings
Berberine
Berberine HCl
Berberine HCl
500 mg
Other ingredients: Vegetable capsule (modified cellulose), Cellulose, Calcium laurate, Silicon dioxide
Certifications
Benefits
Warnings


