

Integrative Therapeutics
Berberine 500 mg by Integrative Therapeutics
60 capsules · 60-day supply
Supports Healthy Blood Sugar Levels and Metabolic Function$32.99
Purchase options
Practitioner-grade brand3rd-party testedFree shipping $50+
Vegan·Vegetarian·Gluten Free·Soy Free·Dairy Free·Milk Free·
Integrative Therapeutics Berberine overview
If you’re looking at berberine for blood sugar, this fits adults with elevated fasting glucose, a higher Hemoglobin A1c, or noticeable post‑meal spikes on a CGM. It’s also useful if triglycerides are high or your Omega-3 Index is low and you’re working on metabolic health. People with insulin resistance, including some with PCOS, often see the most value. At 500 mg per capsule, taking it two to three times daily is a clinical dose; if your A1c is already well controlled, this is more maintenance than repletion.
Berberine activates AMPK, the cell’s energy gauge that tells the body to burn fuel and dial back sugar production. By nudging the liver to make less glucose and helping muscles take up more, it smooths post‑meal rises and can lower Hemoglobin A1c within 8 to 12 weeks. It also reduces how much fat the liver exports as VLDL particles (the form that shows up as triglycerides), with typical triglyceride drops of 15–25% in responders and small reductions in hs-CRP (an inflammation marker).
Take one capsule with meals, two to three times per day, because berberine blunts the post‑meal glucose rise best when timed with food. If you’re new to berberine, start with once daily for 3 to 5 days, then add a second dose, and a third if needed. Most glucose changes appear in 2 to 4 weeks, lipids in 8 to 12. Dihydroberberine is an alternative form used at lower doses, but berberine HCl is the form most trials use.
Berberine can add to the effects of diabetes drugs (metformin, insulin, sulfonylureas), so watch for low glucose and adjust with your clinician. It inhibits P‑glycoprotein and CYP3A4 (drug‑processing pathways), which can raise levels of cyclosporine, tacrolimus, and digoxin—skip it if you’re on transplant or narrow‑therapeutic‑index meds unless your specialist is monitoring levels. Avoid in pregnancy and breastfeeding due to risk of newborn jaundice. If your ALT or AST are already elevated, get baseline liver tests and recheck.
Expect mild GI effects (bloating, soft stool) in the first week; taking with food and titrating helps. Berberine and metformin can be used together, but you’ll need closer glucose monitoring. If weight loss happens, it’s usually modest over 2 to 3 months and tracks with better diet and activity. Track Hemoglobin A1c, fasting glucose, fasting insulin, and triglycerides to see if it’s working.
Frequently asked questions
How long does berberine take to lower A1c?
Most people who respond see A1c start to drop by 8 to 12 weeks. Post‑meal glucose can improve in 2 to 4 weeks. Recheck Hemoglobin A1c after 3 months to confirm benefit.
What is the best berberine dose for blood sugar?
Clinical studies commonly use 1,000–1,500 mg per day split with meals. This product delivers 500 mg per capsule, so two to three daily doses hit that range.
Can I take berberine with metformin or GLP‑1 meds?
Yes, but monitor closely. Berberine can add to glucose‑lowering, increasing hypoglycemia risk with insulin or sulfonylureas. Discuss dose adjustments with your clinician.
Does berberine help triglycerides and cholesterol?
It often lowers triglycerides 15–25% in responders over 8–12 weeks, with small improvements in LDL and HDL. Check a lipid panel to verify your response.
Should I take berberine with food or on an empty stomach?
With food is best. Taking it at mealtimes better targets the post‑meal glucose rise and reduces stomach upset like cramping or loose stools.
Is berberine safe long term?
Data up to 6–12 months look reassuring when labs are monitored. If you plan longer use, check Hemoglobin A1c, liver enzymes (ALT, AST), and lipids every 3–6 months.
Who should avoid berberine?
Avoid in pregnancy and breastfeeding, and if you take transplant meds (cyclosporine, tacrolimus) or digoxin unless levels are being monitored. Talk to your specialist first.
What are common side effects of berberine?
The most common are GI: bloating, gas, and softer stools, usually improving after a week. Taking with meals and gradual titration reduce these effects.
How to take it & ingredients
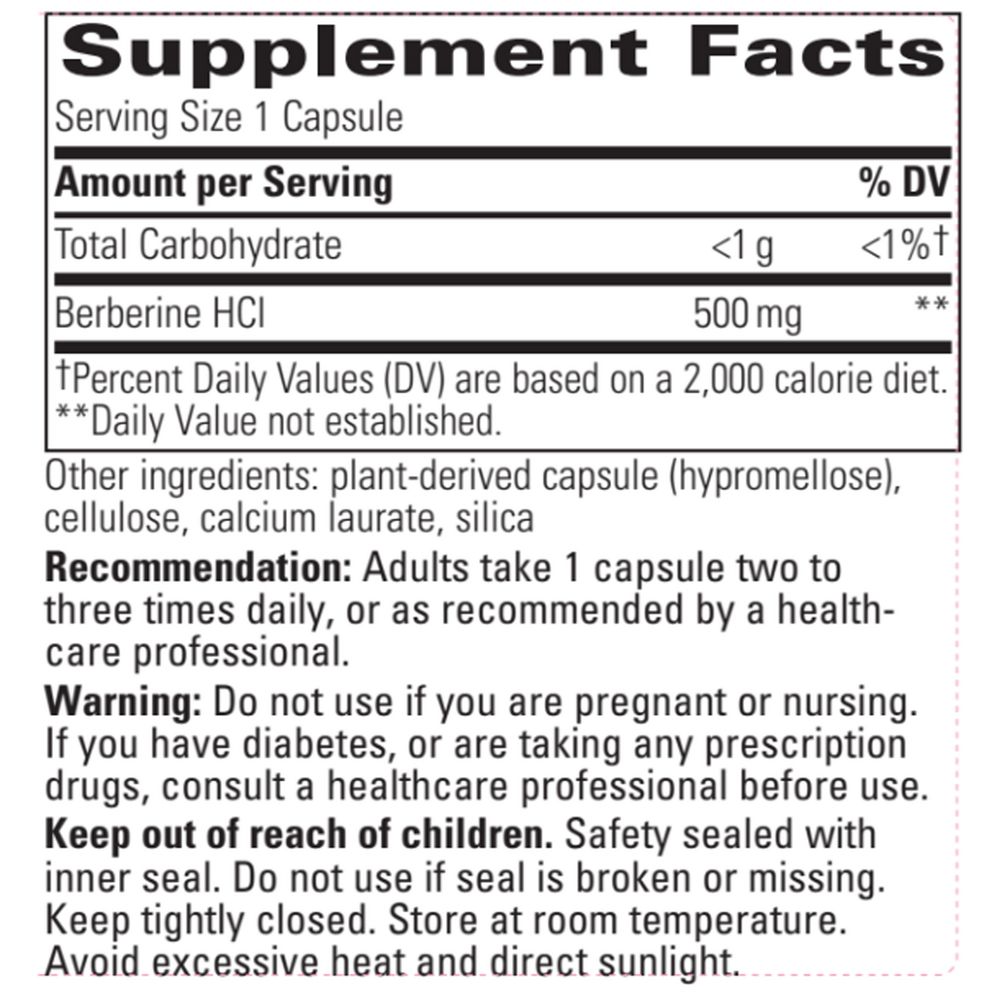
Suggested use: Take 1 capsule two to three times daily, or as recommended by your healthcare professional.
Active ingredients
1 capsule per serving · 60 servings
Berberine
Berberine HCl
Berberine HCl
500 mg
Other ingredients: Vegetable capsule (modified cellulose), Cellulose, Calcium laurate, Silicon dioxide
Certifications
Benefits
Warnings


