


Jigsaw Health
MagSRT by Jigsaw Health
240 tablets · 60-day supply
Sustained Release Magnesium for Energy, Muscle Function & Relaxation$49.99
Purchase options
Practitioner-grade brand3rd-party testedFree shipping $50+
Vegan·Gluten Free·Soy Free
Jigsaw Health MagSRT overview
If your Magnesium, RBC is low or in the lower end of normal and you feel tight muscles, low energy, or restless sleep, magnesium malate is a practical next step. It’s a fit for athletes who cramp after hard sessions, heavy coffee users, people under chronic stress, and those on diuretics or proton‑pump inhibitors who often run low. The 500 mg elemental magnesium here is a higher, repletion‑leaning dose; if you only need maintenance, lower‑dose magnesium glycinate or citrate can be enough. Vegans and light eaters who miss nuts, legumes, and greens also tend to benefit.
Dimagnesium malate provides magnesium plus malic acid (a Krebs cycle fuel your cells use to make ATP, the molecule that carries energy). This pairing supports muscle relaxation and steadier energy, while the 8‑hour time release spreads absorption to reduce the laxative effect common with fast‑release forms. Compared with magnesium oxide (poorly absorbed) or citrate (effective but looser stools), magnesium malate is gentler at higher doses. The added P5P (the active form of vitamin B6), L‑5‑MTHF (the methylated folate your body can use directly), and methylcobalamin (an active B12) aid enzyme reactions that use magnesium and help keep homocysteine (a sulfur amino acid tied to methylation and vascular health) in a good range.
Take four tablets per day with food, as labeled for Jigsaw Health MagSRT. Many patients do best splitting the dose, breakfast and dinner, to smooth levels and minimize bowel changes. Expect sleep, muscle, or energy changes within 1 to 3 weeks; lab shifts in Magnesium, RBC typically show up by 4 to 8 weeks. If you’re already regular or prone to loose stools, start with half the dose for a week, then increase as tolerated.
Magnesium binds certain medications and can reduce their absorption. Separate by at least 2 hours from levothyroxine, and by 4 hours from tetracycline or fluoroquinolone antibiotics and from bisphosphonates (bone drugs). It can also compete with iron—take iron at a different time of day. If you have significant kidney disease, or take high‑dose magnesium from multiple products, check levels and dose with your clinician to avoid buildup.
Frequently asked questions
Is magnesium malate better than magnesium glycinate for sleep?
Both can help if you’re low in magnesium. Glycinate is often favored at bedtime because it’s very calm on the gut. Malate pairs magnesium with malic acid for energy production, which some prefer earlier in the day. Choose based on tolerance and how you feel.
How long does magnesium malate take to work?
Symptoms like muscle tightness or sleep quality can improve within 1–3 weeks. Measurable changes in Magnesium, RBC usually appear by 4–8 weeks. Consistent daily dosing matters more than time of day.
Will magnesium malate cause diarrhea?
It’s less likely than citrate because this is sustained‑release, but any magnesium can loosen stools at higher doses. Splitting the dose with meals and titrating up over a week reduces that risk.
Can I take magnesium with antidepressants or blood pressure meds?
Generally yes, but separate from medications by 2 hours to avoid binding in the gut. If you take tricyclics, lithium, or multiple blood pressure drugs, discuss dosing with your prescriber, as magnesium can have mild blood pressure–lowering effects.
Can I crush MagSRT tablets?
No. Crushing defeats the sustained‑release design and raises the chance of GI side effects. If you have trouble swallowing tablets, consider a powdered magnesium glycinate or citrate instead.
Is magnesium malate safe in pregnancy or breastfeeding?
Magnesium is commonly used in pregnancy, but high doses should be individualized. Review your total daily magnesium from diet and prenatals with your obstetric clinician before adding a separate 500 mg dose.
What labs should I check while taking magnesium?
Magnesium, RBC is more informative than Magnesium, Serum for body stores. If you’re using B‑vitamin–containing formulas, Homocysteine and Vitamin B12 can add context. Recheck after 4–8 weeks of steady dosing.
How to take it & ingredients
Suggested use: As a dietary supplement, take 4 tablets per day with food. Divide doses if desired or as directed by your healthcare provider.
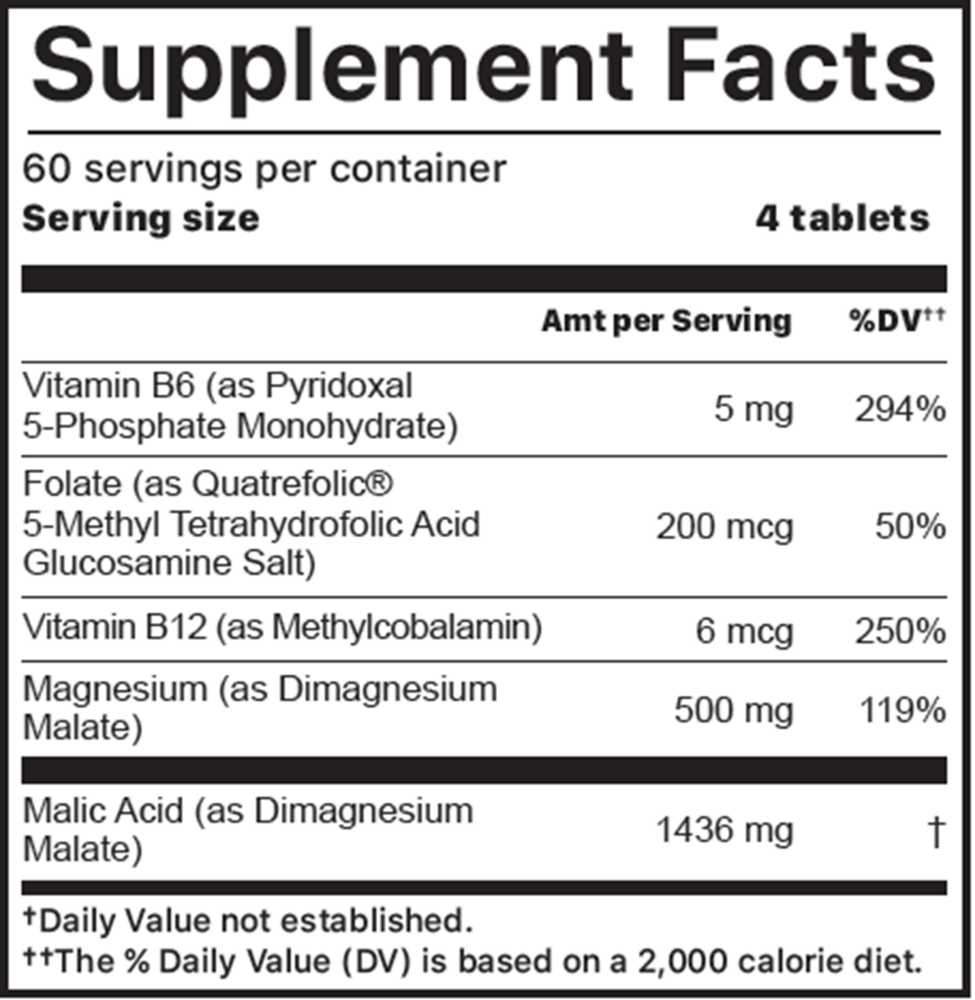
Active ingredients
4 tablets per serving · 60 servings
Magnesium
Dimagnesium malate
Dimagnesium malate
500 mg
Malic Acid
From dimagnesium malate
From dimagnesium malate
1436 mg
Vitamin B6
Pyridoxal 5-phosphate monohydrate
Pyridoxal 5-phosphate monohydrate
5 mg
Folate
Quatrefolic 5-methyl tetrahydrofolic acid glucosamine salt (L-5-MTHF)
Quatrefolic 5-methyl tetrahydrofolic acid glucosamine salt (L-5-MTHF)
200 mcg
Vitamin B12
Methylcobalamin
Methylcobalamin
6 mcg
Other ingredients: Microcrystalline cellulose, Hydroxypropyl cellulose, Croscarmellose sodium, Hydroxypropyl methylcellulose (plant-based fibers for sustained release), L-leucine, Silicon dioxide, Clear coating (hydroxypropyl methylcellulose and sunflower oil), Micro wax
Certifications
Benefits
Warnings
Customers also considered

Ortho Molecular Products
CereMag
99 grams
$77.76extra 10% off with Subscribe & Save

Garden of Life
Dr. Formulated Magnesium Raspberry
197.4 grams
$24.99extra 20% off with Subscribe & Save

Natura Health Products
Dual-Mag Complex
90 capsules
$22.99extra 22% off with Subscribe & Save

Ortho Molecular Products
Mag Threonate
60 capsules
$78.64extra 10% off with Subscribe & Save