

Metagenics
OmegaGenics EPA-DHA 1000 Fish Oil 1400 mg by Metagenics
120 softgels · 120-day supply
Premium Omega-3 Support for Heart, Brain, and Joint Health$XX.XX$83.99retail
This item is currently out of stockGet notified when this item is back in stock
20% below MSRP3rd-party tested for purity & potencyFree shipping $50+
Gluten Free
Metagenics OmegaGenics EPA-DHA 1000 Fish Oil overview
If you’re searching for fish oil for high triglycerides, this is the lane where omega-3s shine. Adults with elevated Triglycerides, a low Omega-3 Index, or little seafood intake often see the most benefit. The roughly 1,000 mg of EPA+DHA per softgel is a clinically relevant dose for lipid work; many people need two to three daily for triglyceride reduction, then step down for maintenance once labs improve.
EPA and DHA reduce how much fat your liver packages into VLDL particles (the carriers that show up on a lipid panel as triglycerides), and they nudge cells to burn fatty acids for energy. Most responders see triglycerides drop 20–30% within 4 to 12 weeks. These fats also shift membrane signaling toward fewer pro-inflammatory eicosanoids (short-lived chemical messengers), which is why hs-CRP, an inflammation marker, sometimes falls.
Take with meals to improve absorption and cut fishy burps. For triglycerides, higher daily totals of EPA+DHA are typically used short term, then a maintenance dose follows once Triglycerides and the Omega-3 Index improve. Splitting doses across breakfast and dinner works well. If you’re targeting brain or joint comfort rather than lipids, a steady daily maintenance dose is reasonable.
If you use blood thinners like warfarin, apixaban, or clopidogrel, or high-dose aspirin, talk to your clinician before adding high-dose omega-3s, as they can mildly increase bleeding time. A history of atrial fibrillation (irregular heartbeat) warrants a conversation too, since some high-dose trials in heart patients signaled more episodes. Fish allergy, planned surgery, or prescription icosapent ethyl are other reasons to check in first.
Strict vegans will want an algae-based omega-3 instead. If your Triglycerides are extremely high with pancreatitis risk, you need clinician-directed care; fish oil can be part of the plan but isn’t first aid. Concerned about contaminants? Reputable fish oil is molecularly distilled and batch-tested for heavy metals and PCBs—ask for verification if you don’t see it.
Frequently asked questions
How long does fish oil take to lower triglycerides?
Most responders see meaningful triglyceride reductions within 4 to 12 weeks at clinically dosed EPA+DHA. Recheck a fasting lipid panel after 8 to 12 weeks and adjust the dose or diet based on the result.
Does fish oil thin your blood?
At typical doses, omega-3s have a mild antiplatelet effect, which can slightly increase bleeding time. It’s usually not clinically important, but if you’re on warfarin, apixaban, clopidogrel, or have surgery planned, discuss dosing with your clinician.
What’s the difference between EPA and DHA?
EPA is more active for triglyceride lowering and inflammation signaling. DHA is key for brain and eye membranes. Many people use a blend for broad coverage; very high triglycerides are often targeted with higher EPA relative to DHA.
Can I take fish oil with a statin?
Yes. Omega-3s and statins are commonly used together: statins address LDL cholesterol, while EPA+DHA target triglycerides. Monitor your lipid panel to see the combined effect and fine-tune dosing with your clinician.
Will this cause fishy burps or reflux?
Taking softgels with meals, splitting doses, or briefly chilling capsules can reduce burps. Persistent reflux often improves by lowering single-dose size and spreading intake across the day.
Is krill oil better than fish oil?
For triglyceride reduction, outcome data favor clinically dosed EPA+DHA regardless of source. Krill oil delivers less EPA+DHA per capsule, so it’s harder to reach effective totals without many capsules.
Which labs should I check while taking fish oil?
Track Triglycerides on a fasting lipid panel and consider the Omega-3 Index to confirm tissue levels. If you’re aiming for inflammation changes, hs-CRP is a reasonable marker to follow.
Is mercury a concern with fish oil?
Quality fish oils are purified and batch-tested to remove heavy metals like mercury and industrial contaminants. Choose brands that disclose third-party testing or certifications for purity.
How to take it & ingredients
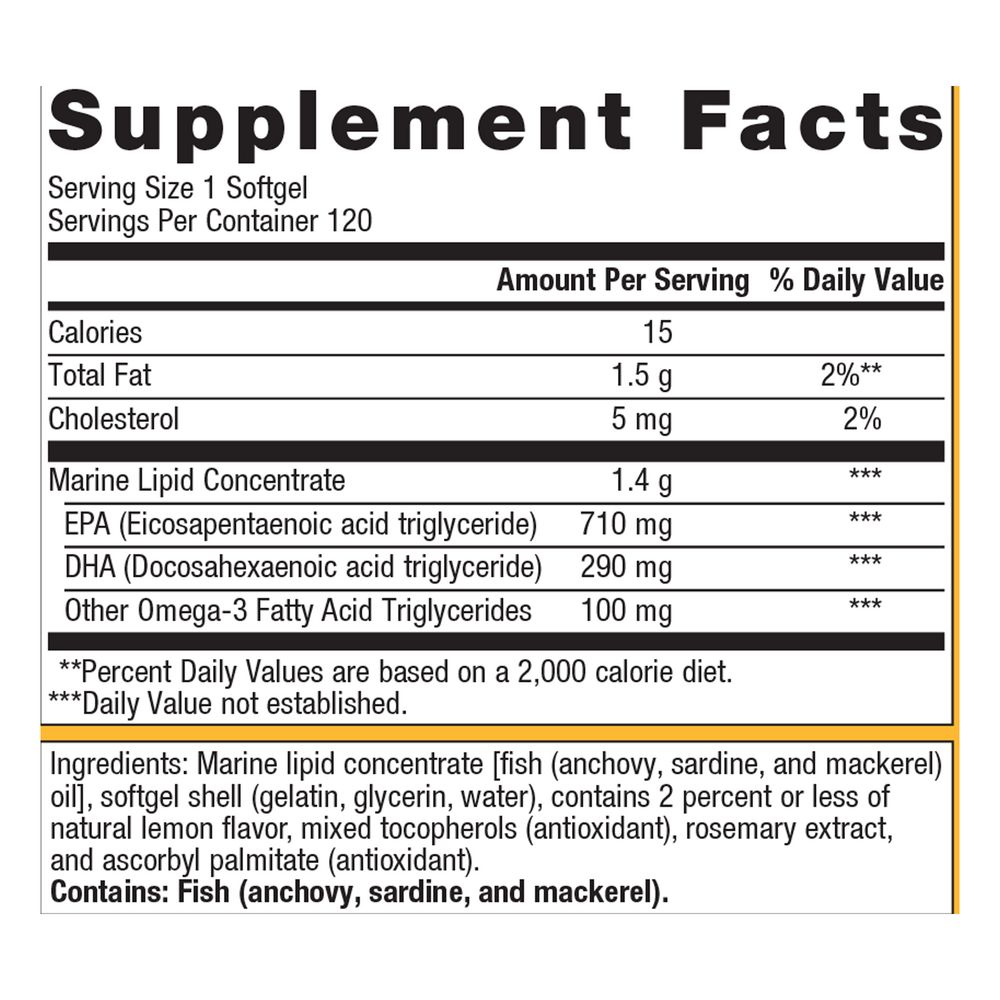
Suggested use: Take one softgel up to three times daily with food or as directed by your healthcare practitioner.
Active ingredients
1 softgel per serving · 120 servings
▼
Omega-3 Fatty Acids
Marine Lipid Concentrate
Marine Lipid Concentrate
1400 mg
EPA
Eicosapentaenoic acid triglyceride
Eicosapentaenoic acid triglyceride
710 mg
DHA
Docosahexaenoic acid triglyceride
Docosahexaenoic acid triglyceride
290 mg
Other Omega 3 Fatty Acid Triglycerides
100 mg
Other ingredients: Fish oil (anchovy, sardine, mackerel), Softgel shell (gelatin, glycerin, water), Natural lemon flavor, Mixed tocopherols, Rosemary extract, Ascorbyl palmitate
Certifications
Benefits
Warnings
Customers also considered

Thorne
Advanced DHA
60 gelcaps
$XX.XX$30.00retail
Add to cart to see your price

Garden of Life
Dr. Formulated Advanced Omega
60 softgels
$XX.XX$31.99retail
Add to cart to see your price
Garden of Life
Dr. Formulated DHA 1g
30 softgels
$XX.XX$31.99retail
Add to cart to see your price
Garden of Life
Dr. Formulated Prenatal DHA
30 softgels
$XX.XX$29.99retail
Add to cart to see your price